
Case of the week
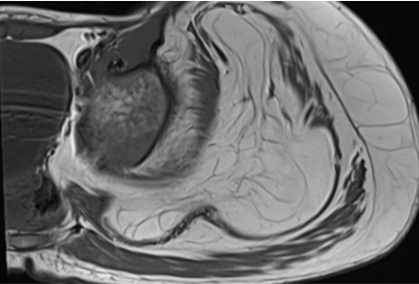
2 years old male presented with progressive disproportionate enlargement of left thigh, leg, foot and hand.
2 years old male presented with progressive disproportionate enlargement of left thigh, leg, foot and hand.
View Case
A 54 years old, male patient presented with complaints of swelling in the bilateral lower limbs and breathlessness.
A 54 years old, male patient presented with complaints of swelling in the bilateral lower limbs and breathlessness.
View Case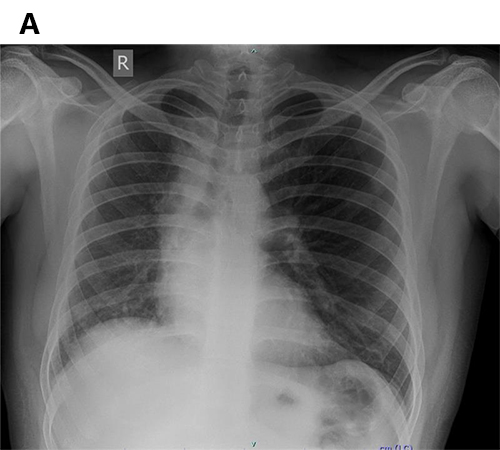
37 year old male presented with sudden loss of consciousness following nocturnal micturition with abnormal screening chest X- ray.
37 year old male presented with sudden loss of consciousness following nocturnal micturition with abnormal screening chest X- ray.
View Case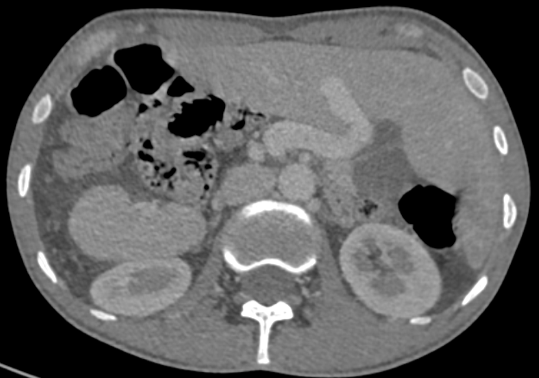
A 27 year old gentleman presented with few episodes of hemoptysis. He also had a history of cough with expectoration since few months.
A 27 year old gentleman presented with few episodes of hemoptysis. He also had a history of cough with expectoration since few months.
View Case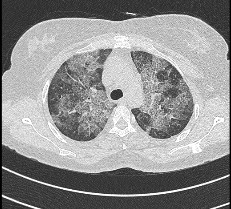
Walk in OPD patient with History of on and off mild breathlessness and fever since 6 months.
Walk in OPD patient with History of on and off mild breathlessness and fever since 6 months. No history of tuberculosis or ICU admission.
View Case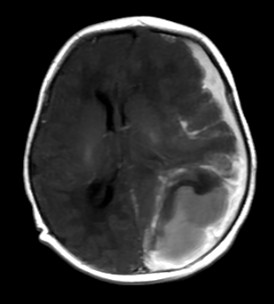
5 days old infant presented with history of seizure. History of prolonged difficult delivery present.
5 days old infant presented with history of seizure. History of prolonged difficult delivery present.
View Case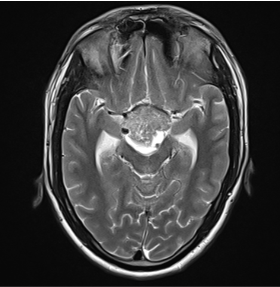
A 18 year old male, History of headache since 1 month. Change of voice since 1 month.
A 18 year old male, History of headache since 1 month.Change of voice since 1 month.
View Case
75y old male presented with numbness in right upper limb since 1 day associated with slurring of speech
75y old male presented with numbness in right upper limb since 1 day associated with slurring of speech
View Case