
2 years old male presented with progressive disproportionate enlargement of left thigh, leg, foot and hand.
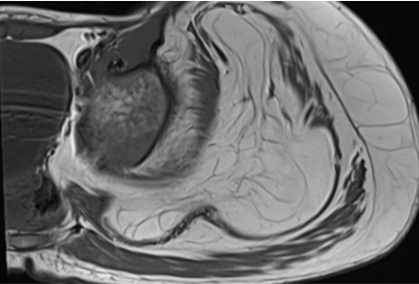
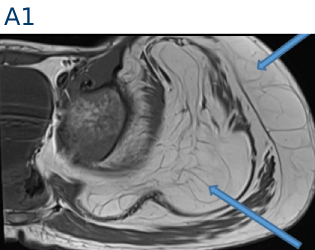
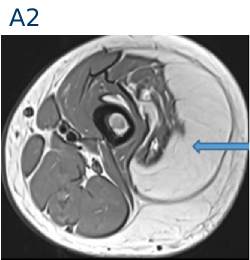
A. FINDINGS – MR LEFT LEG
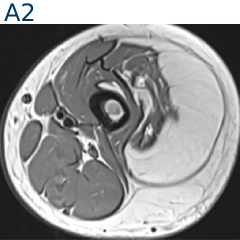
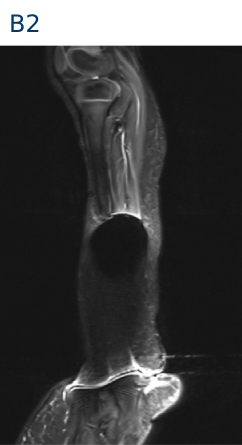
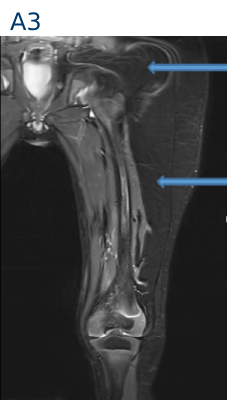
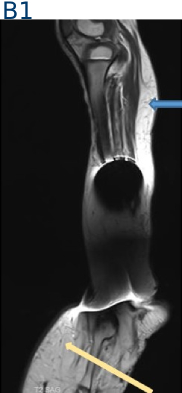
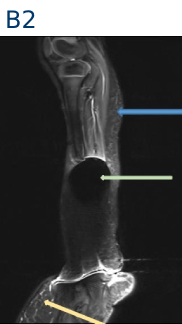
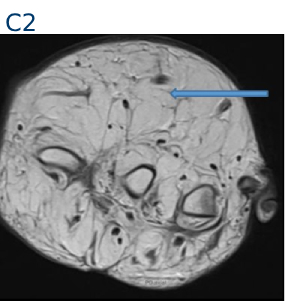
B. FINDINGS – MR LEFT LEG
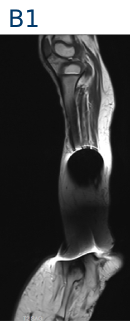
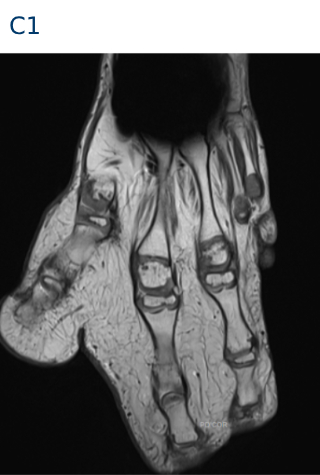
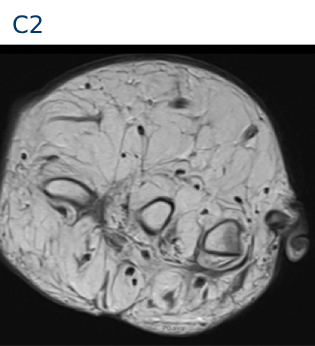
C. FINDINGS – MR LEFT HAND
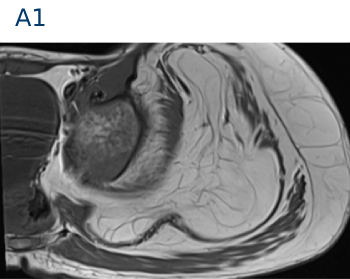

- Large lipomatous hypertrophy of left gluteal region and the thigh, involving both muscular and subcutaneous planes. The lipomatous tissue is decussating between the fibers of gluteus medius, minimus and muscles of lateral compartment of thigh.
- The involved muscles appear atrophied.
- Hypertrophy of subcutaneous fat in the leg (blue arrow)
- Similar lipomatous hypertrophy is seen in visualized foot (yellow arrow)
- Susceptibility artefact is seen obscuring lower leg - likely due to prior surgical history (green arrow)
- Similar lipomatous hypertrophy of hand (blue arrow)
- Soft tissue syndactyly, digital gigantism and macrodactyly involving 1st, 2nd and 3rd digits (green arrow)
- Fourth and fifth digits, including the metacarpals and phalanges are hypoplastic(yellow arrow)

Macrodystrophia lipomatosa
- Rare non hereditary congenital developmental anomaly characterized by progressive overgrowth of mesenchymal elements with a disproportionate increase in fibroadipose tissue involving nerve sheath, muscle, periosteum and bone marrow.
- Occurs most frequently along the median nerve distribution in the upper extremities and the plantar nerve in the lower extremities.
- Usually, one or more digits of the unilateral limb are affected.
- May be associated with syndactyly, polydactyly, brachydactyly or clinodactyly.
- Static form - the growth rate of affected tissues is normal.
- Progressive form - the growth rate of mesenchymal tissues is faster when compared with normal tissues and ceases its abnormal growth at puberty.
Etiopathogenesis
- Lipomatous degeneration
- Fetal circulation abnormality
- Damage of extremity bud and alteration of somatic cells in intrauterine life
Complications
- Secondary osteoarthritis
- Compression of neurovascular structures causing impairment of function
- Cosmetic problem
Causes of macrodactyly
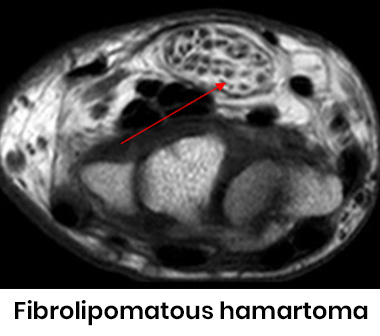
| Fibrolipomatous hamartoma | Mostly affects median nerve, digital overgrowth, speckled appearance on MR |
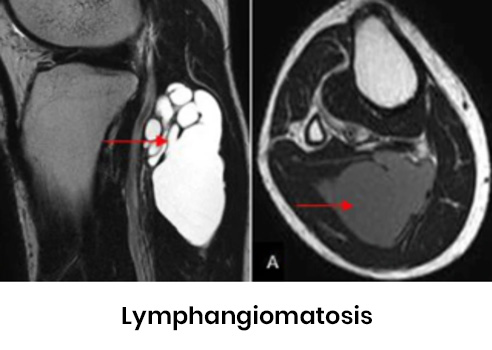
| Lymphangiomatosis | Increased lymphatic channels, pitting edema T1 hyperintense (to muscles) and T2 hypointense (to fat), lytic bone lesions, no osseous growth. |
|
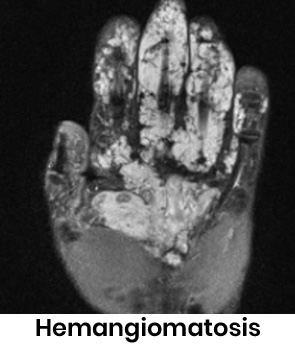
Hemangiomatosis |
Increased vascular channels, bluish lesions Worm like T2/STIR hyperintense areas, no osseous growth. |
Causes of macrodactyly
| Klippel-Trenaunay-Weber syndrome | Port Wine stain Osseous and soft tissue hypertrophy, venous malformation |
| Maffucci/ Ollier's syndrome | Expansile lytic lesions in phalanges. |
| Proteus syndrome | Hemihypertrophy with asymmetrical partial gigantism, pigmented nevi, lung cyst, extensive lymphangitic and vascular malformation. |


REFERENCES
Mehra R, Bhartiya R, Agrawal P, Kumari N. Macrodystrophia Lipomatosa: Clinico-patho-radiological Correlation. Indian J Med Paediatr Oncol. 2017 Oct-Dec;38(4):559-562. doi: 10.4103/ijmpo.ijmpo_65_16. PMID: 29333032; PMCID: PMC5759084.
Dr KAMESH G
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr SHIKHA JOSHI
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
