
7 year old male child presented with complaints of walking on toes and swelling over left lower limb joints. No history of trauma.
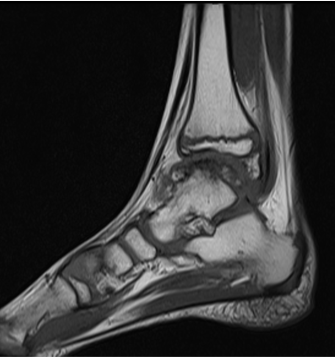
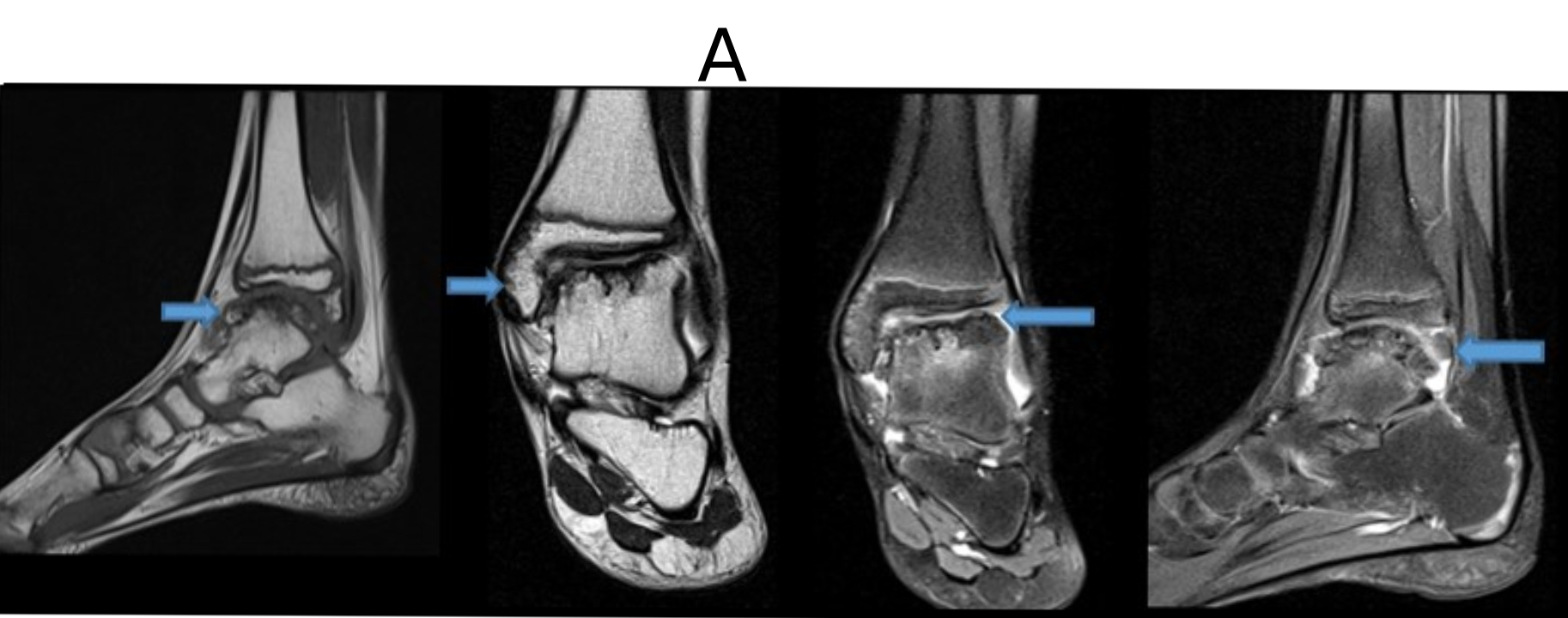
A. FINDINGS – MR ANKLE JOINT
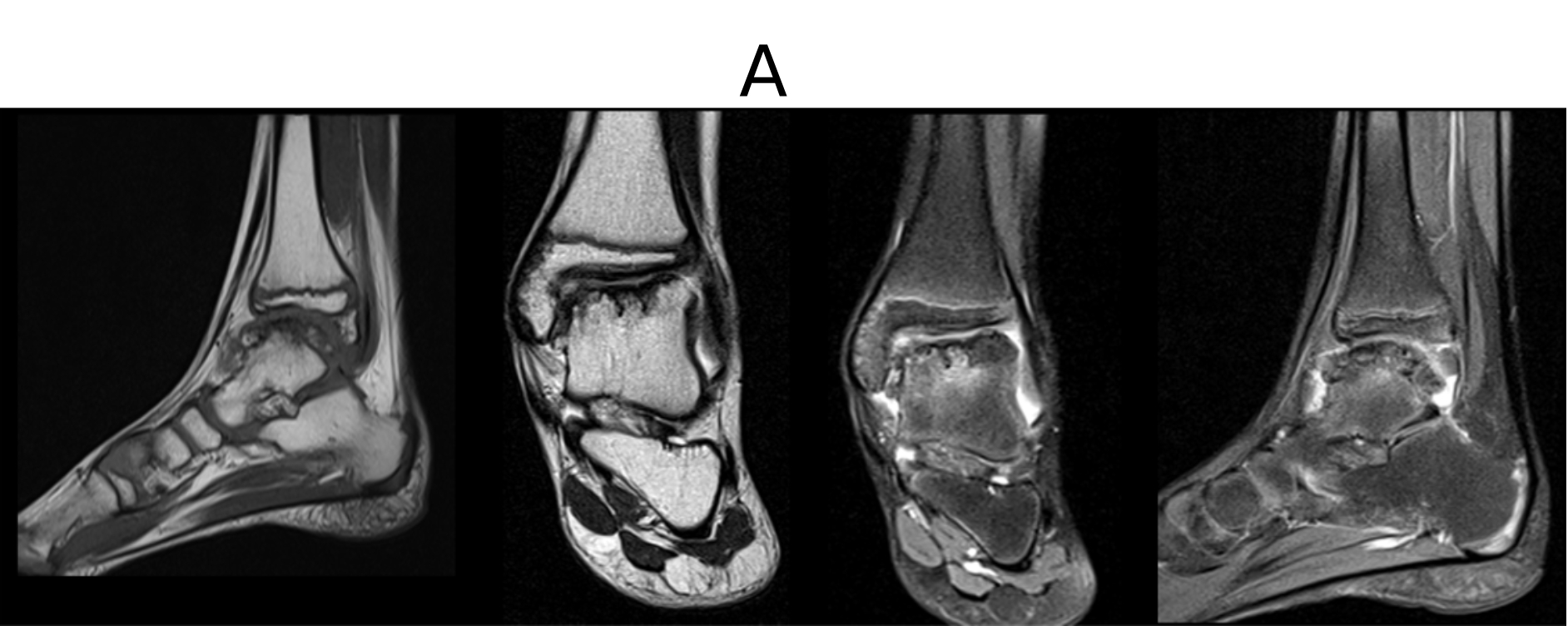
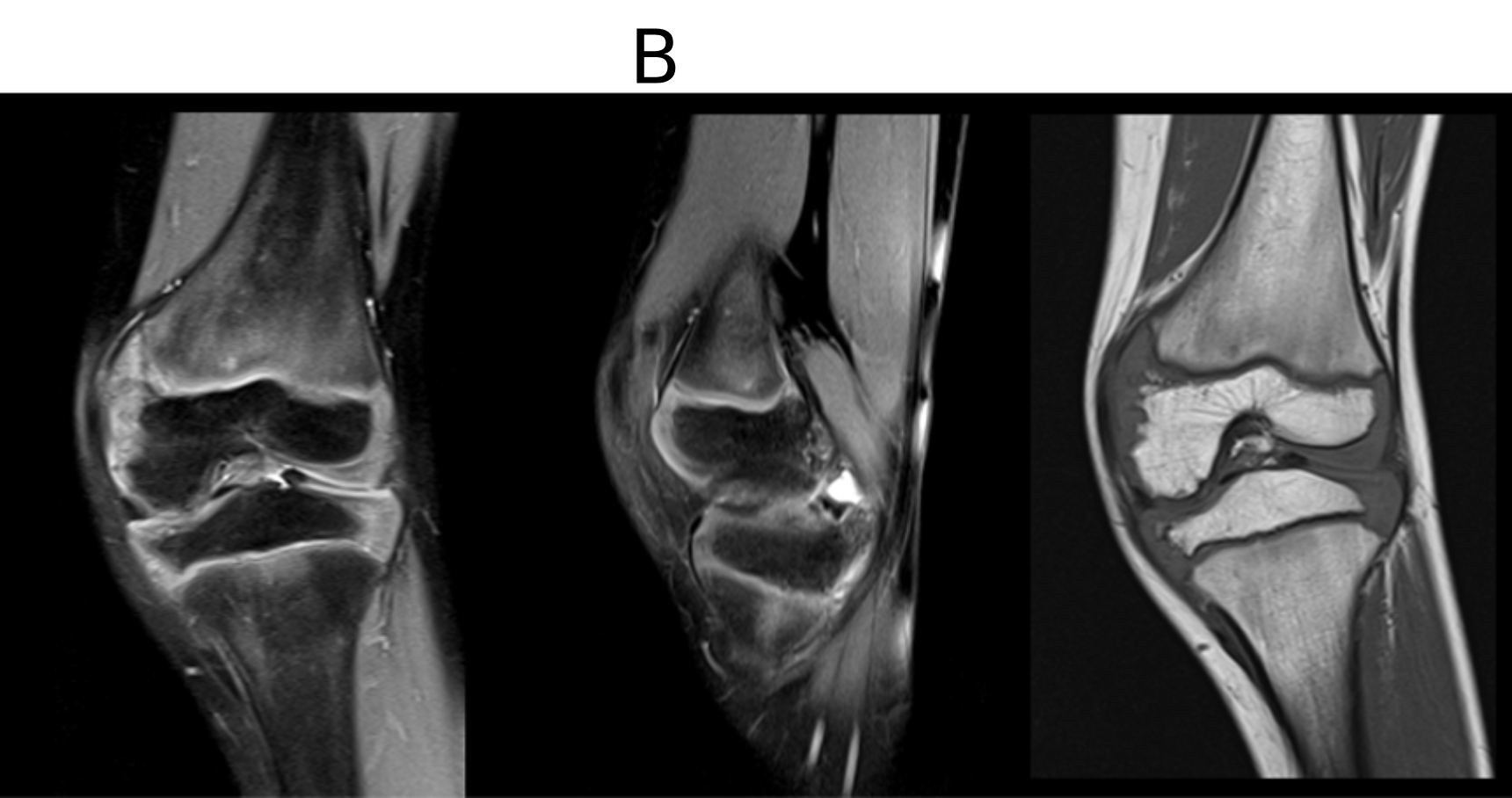
B. FINDINGS – MR KNEE JOINT
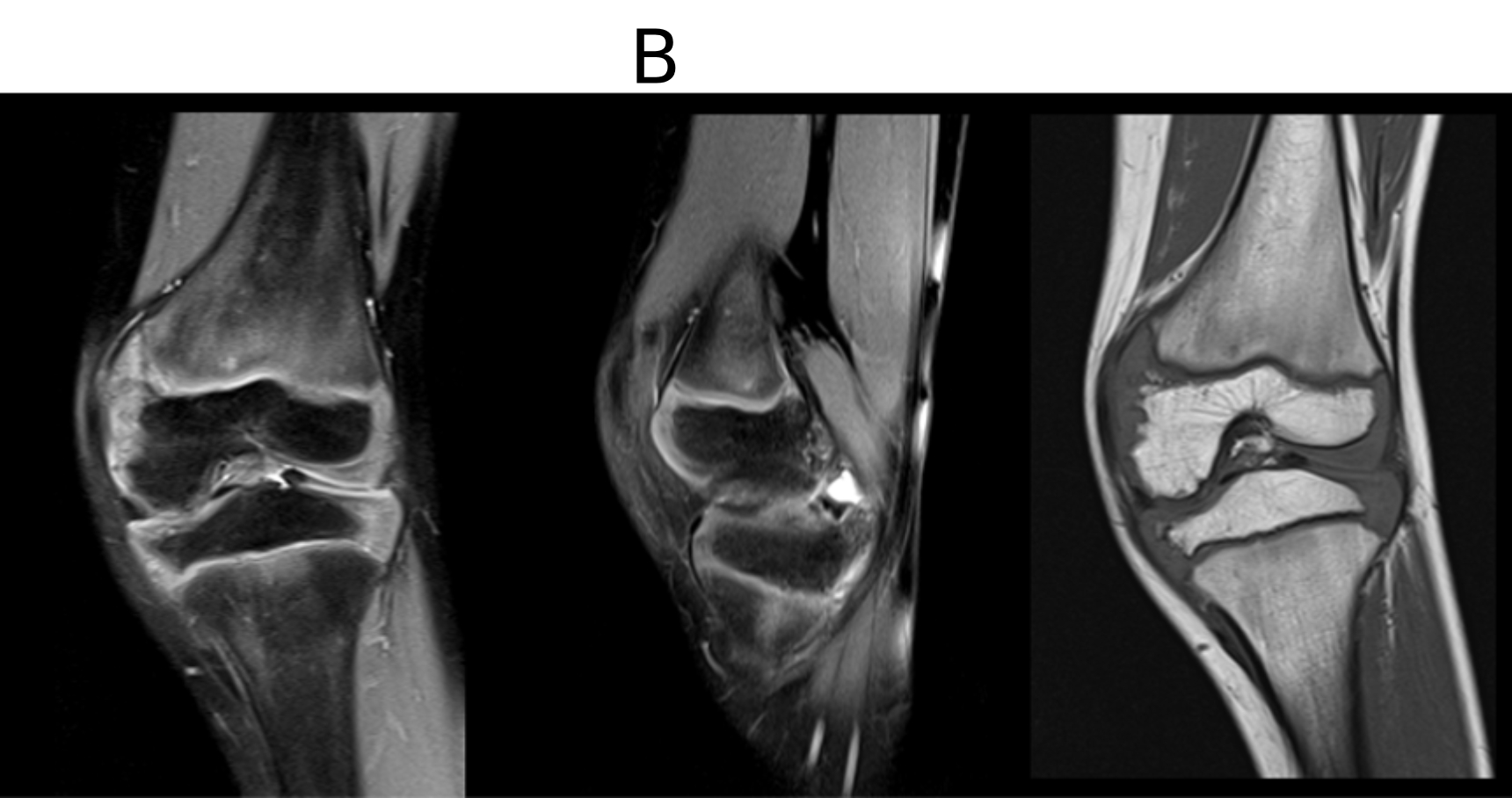
A. LEGENDS
- Cortical irregularity with epiphyseal over growth, marrow edema is seen involving distal medial epiphysis of tibia and medial malleolus.
- Cortical irregularity with epiphyseal over growth few ossified mass and marrow edema seen involving dome of talus.
- Few irregular ossified T1 hypointense masses with reduced tibio-talar joint space.
- Mild joint effusion noted
B. LEGENDS
- Reduced bilateral (medial>lateral) tibio-femoral joint space with genu valgus.
- Cortical irregularity with epiphyseal overgrowth, with few extra-osseous ossifications involving bilateral (medial > lateral) distal femoral condyles and tibial plateau.
- Mild marrow edema in bilateral (medial>lateral) distal femoral condyles, tibial plateau and proximal fibular epiphysis.
- Fibular epiphysis is grossly Normal.
DIAGNOSIS :
- Imaging features are suggestive of Trevor’s disease (Dysplasia epiphyeaslis hemimalacia).
DISCUSSION :
- Characterized by epiphyseal over-growth and osteocartilaginous epiphyseal lesions caused by idiopathic benign cell proliferation, dysplasia epiphysealis hemimelica (DEH), also known as Trevor disease, is an infrequently reported clinical entity that may manifest with painless deformity, limited range of motion, mechanical pain, and localized growth disturbances.
- It is likely that many of these cases are misdiagnosed as osteochondromas or other disease entities or are asymptomatic, making DEH more common than has been reported in the past. Male patients are predominantly affected.
- DEH generally entails unilateral involvement of an epiphysis or epiphyseal equivalent (e.g., calcaneus, talus, patella, ischium, pubic bone, and carpal bones) or multiple epiphyses within one extremity.
- Classically, involvement may occur in a hemimelic distribution involving multiple joints on the same side of the extremity, with the medial side more often involved.
- Symptoms are largely dependent on the size and location of the epiphyseal lesion, with most patients reporting combinations of deformity, swelling, restricted motion, or mechanical pain.
Pathophysiology :
- In DEH, primarily abnormal development of the epiphyseal cartilage results in abnormal hypertrophy of the epiphyseal cartilage and subsequent excessive ossification.
- DEH is thought to constitute an idiopathic, sporadic epiphyseal overgrowth abnormality without any identifiable hereditary or environmental risk factors
- In DEH, chondrocyte clusters are seen in conjunction with disorganized cartilage, unabsorbed cartilage fragments, and small ossification centers, whereas osteochondromas follow a more orderly, contiguous ossification process that more closely simulates the normal development of the physis.
Classification :
Three types:
- localized DEH, which affects a single bone;
- classic DEH, which involves more than one bone of a single lower extremity in a hemimelic distribution (on the same side of the extremity [i.e., medial versus lateral]
- generalized or severe DEH, which involves an entire lower limb from pelvis to foot.
DIFFERENTIAL DIAGNOSIS :
- Osteochondroma
- Metachondromatosis
- Multiple epiphyseal dysplasia
Dr NEHA SATHYANARAYANA
Radiology resident
MHRG
Dr DEEPTI H V
Senior Consultant Radiologist
MHRG
