
31 yr old female with history of right shoulder and upper arm pain, difficulty in lifting the arm.
- 31 yr old female with history of right shoulder and upper arm pain, difficulty in lifting the arm.
- No history of trauma.


- Image (a): Isointense barely perceptible intramuscular lesion in the long head of triceps.
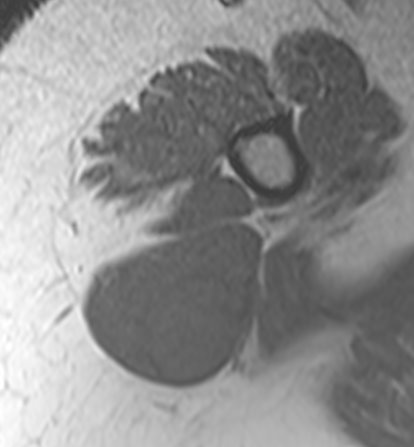
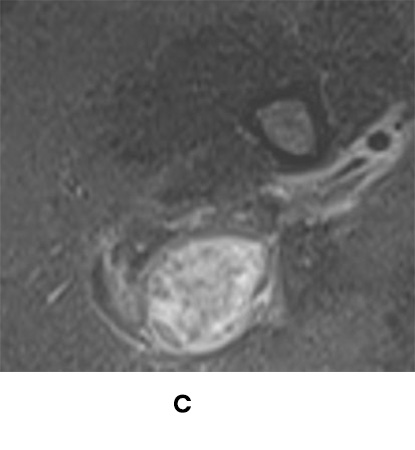
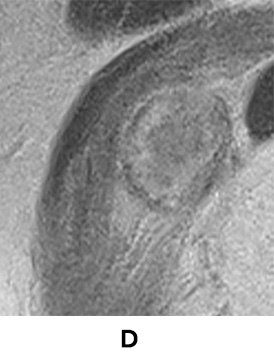
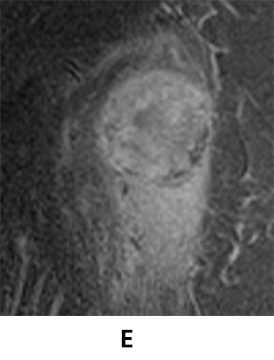
- Image (b, c, d and e): Fairly well circumscribed heterogeneous hyperintense intramuscular lesion with surrounding edema within long head of triceps.
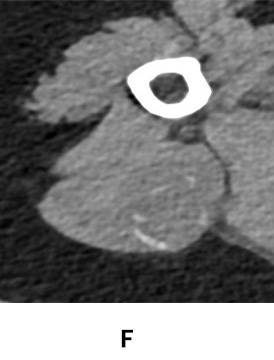
- Image (f): Correlative CT demonstrates discontinuous rim calcification at the periphery of the lesion.
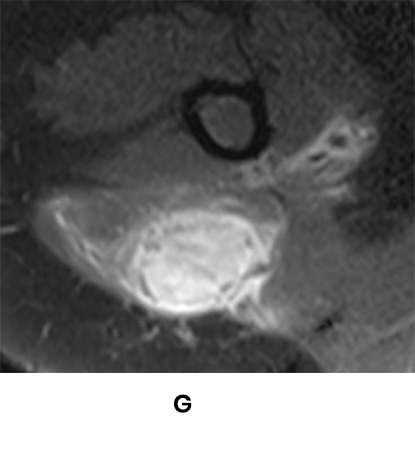
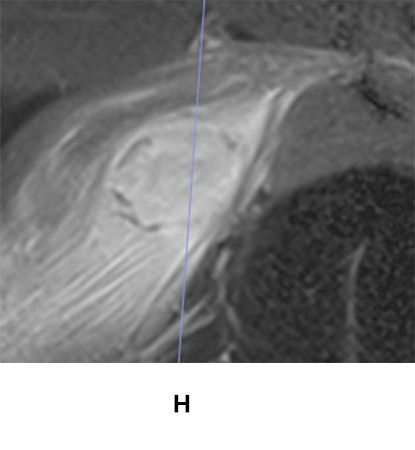
- Image (g, h): Solid post contrast enhancement of the lesion on delayed phase (shown in the image) with enhancement in the surrounding muscle fibres. Discontinuous peripheral hypointense areas corresponding to calcifications on CT is also seen.
- Early-intermediate stage of myositis ossificans involving the long head of triceps with perilesional inflammatory changes.
MYOSITIS OSSIFICANS (MO) :
- MO is a benign, solitary, self-limiting ossifying soft tissue mass typically occurring within the skeletal muscles.
- Lesion is either idiopathic or follows trauma or repetitive microinjury.
- Clinical presentation is pain persisting longer than muscle strain, paraesthesia, weakness and lymphoedema.
- Symptoms usually improve as the lesion matures with minimal or no symptoms of imaged in the late stage of the disease.
Conditions related to MO :
- Myositis ossificans circumscripta: soft tissue new bone formation after trauma.
- Myositis ossificans progressiva: rare inherited disabling condition characterized by progressive ossifications of muscles or tendons.
- Panniculitis ossificans: MO occurring in subcutaneous fat.
- Fibro-osseous pseudotumor of digits: MO occurring in digits.
Imaging findings :
Radiograph and CT:
- Not visible in very early stages.
- Discontinuous and progressive peripheral calcification in a soft tissue lesion.
- In late stages, smaller size and densely calcified intramuscular lesion.
MR IMAGING IN MO :
MR imaging findings varies depending on the stage of the lesion evolution.
Early stage MO :
- T1 hypointense, T2 and STIR hyperintense intramuscular lesion with edema of the surrounding muscle fibres.
- Diffuse post contrast enhancement seen. Peripheral enhancement seen in presence of central non-enhancing hematoma.
- Increased signal intensity of the lesion in an expanded muscle with intact muscle fibres results in a “striate pattern” when images are obtained in a plane parallel to the muscle fibres in T2 or post contrast T1 images.
Intermediate stage MO :
- T1 isointense, sometimes hyperintensity may be seen.
- T2 and STIR heterogeneously hyperintensity. Central fluid signal areas may be present due to haemorrhage.
- Solid heterogeneous enhancement though less than that of early stage lesion.
- Peripherally placed calcifications start appearing on xray or CT. These calcifications appear as peripheral low signal rim like areas on MRI.
Mature/late stage MO :
- Well corticated peripherally calcified lesion.
- Edema starts resolving.
- Heterogeneous signal persists with well-defined peripheral calcification.
- Lesion may appear like native bone.
Differential Diagnosis
Soft tissue sarcoma:
- Perilesional edema is atypical in most sarcomas unless there is a recent intervention or secondary infection.
- Calcifications in sarcoma is typically central whereas in MO it is peripheral.
- Biopsy of MO mimics sarcoma on histopathology due to the presence of osteoid matrix giving a false impression of osteosarcoma.
- Presence of peripheral calcifications and perilesional edema are the imaging clues to differentiate MO from sarcoma.
- Follow up of MO demonstrates typical stages of evolution into rim or densely calcified lesion.
- Typical MO is a skeletal "Do not touch" lesion.
Dr Dayananda Sagar G
Senior Consultant Radiologist, MHRG