

A 54 years old, male patient presented with complaints of swelling in the bilateral lower limbs and breathlessness.
Contrast enhanced CT OF THE THORAX
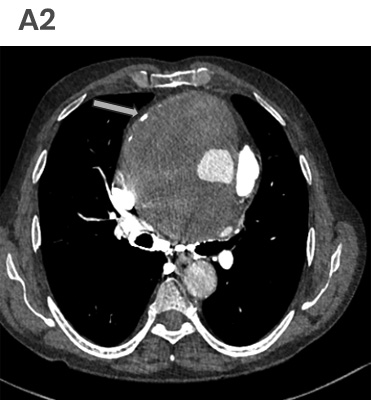
- A. Axial and coronal CECT images at the level of the aortic root and the ascending aorta.
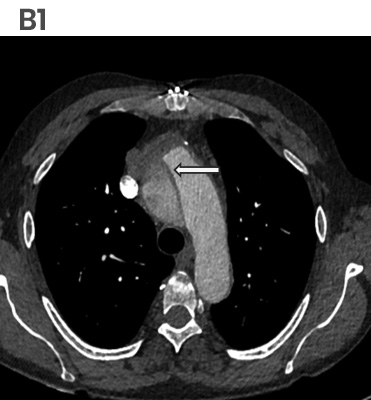
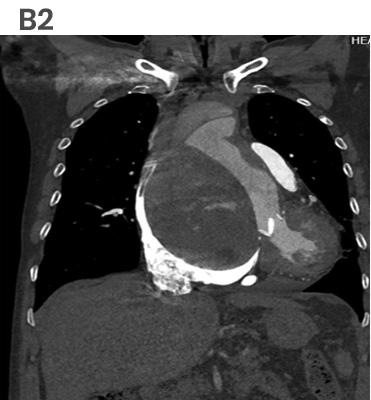
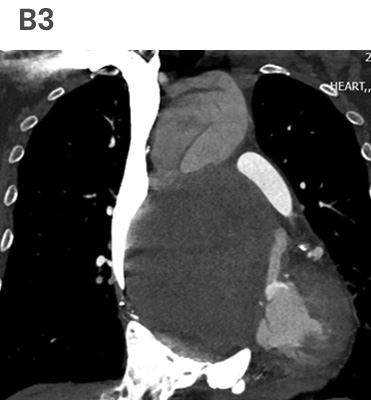
- B. Axial and coronal CECT images at the level of the arch of the aorta.
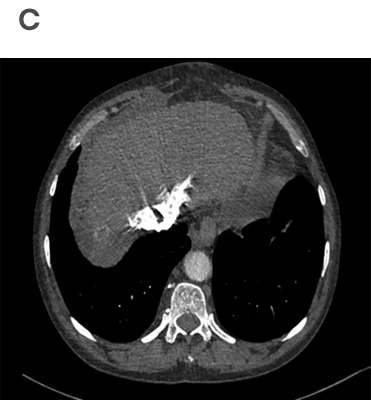
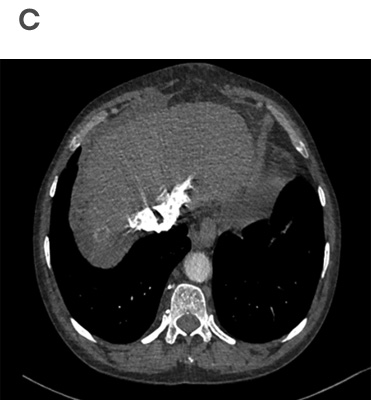
- C. Axial images at the level of the Liver.

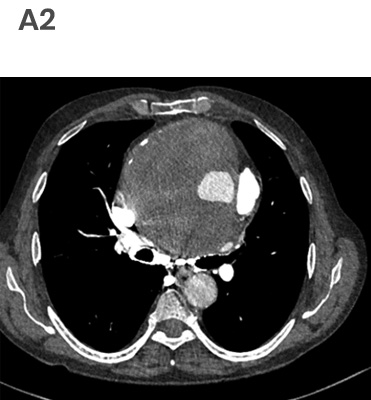
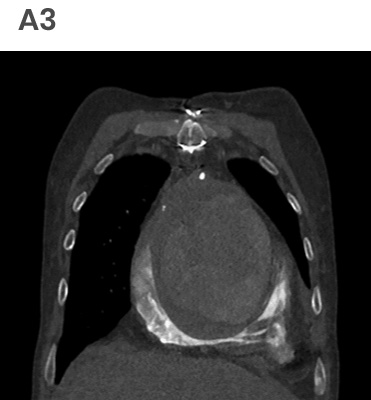

A. Axial and coronal CECT images at the level of the aortic root and the ascending aorta showing
Aneurysmal dilatation at the level of the aortic root and the ascending aorta, with thrombosed lumen and aortic valve prosthesis noted insitu (blue arrow). The aortic wall calcifications (green arrow) are noted at the periphery.Note made of an Intramural hyperdensity (yellow arrow) noted at the level of the aortic root- could represent Intramural thrombus/ Hematoma.
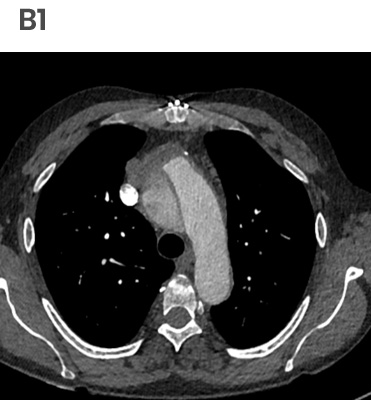
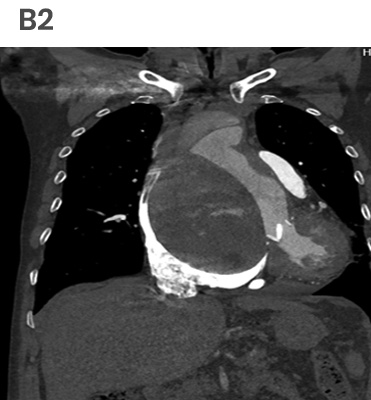
B. Axial and coronal CECT images at the level of the arch of the aorta shows
Stanford A dissection (yellow arrow) at the aortic arch.The dissection segment is noted just distal to the thrombosed aneurysm.The brachiocephalic artery (blue arrow) is seen arising from the true lumen.
C. Axial images at the level of the Liver shows,
Features of right heart strain with reflux of contrast in the iVC and hepatic veins.


Thrombosed aneurysm of the aortic root and the ascending aorta with an intramural hematoma/ thrombus with a Stanford A dissection in the aortic arch and features of right Heart strain.
AORTIC ANEURYSM:
- An aneurysm is defined as a permanent dilatation of the aorta exceeding the normal measurements by more than 2 SDs at a given anatomic level. A diameter equaling or exceeding 1.5 times the expected normal diameter is considered an aneurysm.
- As a rule, Ascending aortic >= 4 cm (in individuals younger than 60 years old), Descending aortic > 3 cm,
- Causes – Atherosclerosis (MC), Cystic median necrosis (ascending aorta) - caused by Marfan syndrome.
Key features for imaging assessment of aneurysms:
- Maximal aortic diameter; shape and extent
- Involvement of aortic branches
- Relationship to adjacent structures, such as the bronchi and esophagus
- Presence of mural thrombus.
- Detection of aortic calcifications.
- In addition, other relevant structures should be carefully evaluated, such as the coronary arteries and the intercostal arterial supply to the spinal cord at the lower thoracic–upper lumbar level.
AORTIC DISSECTION:
Aortic dissection is caused by an intimal tear within an abnormal, weakened vessel wall. This leads to blood entering the wall, with subsequent propagation in the media both proximally and distally, displacing the intima inward.
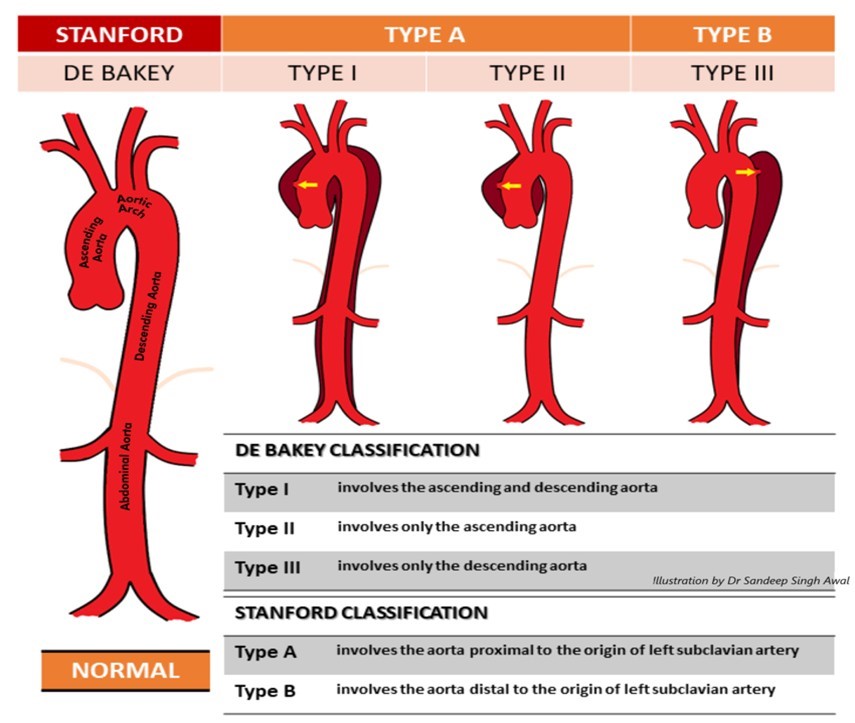
The two well-known classification systems, De Bakey and Stanford.
- The key finding on contrast-enhanced images is an intimal flap separating two lumens.
- The convexity of the intimal flap is usually toward the false lumen that surrounds the true lumen.
- The false lumen usually has slower flow and a larger diameter and may contain thrombi.
- The extent of the thrombus in the false lumen is an indirect indicator of the degree of communication between the true and false lumen, with the false lumen enlarging over time because of intraluminal pressure and wall stress, with risk of aneurysm formation and rupture.
- The major role of MDCT is in providing specific, precise measurements of the extent of dissection, including length, diameter of the aorta and the true and false lumens, involvement of vital vasculature, and distance from the intimal tear to the vital vascular branches.
- The occurrence of an acute aortic dissection following replacement of the aortic valve is well known, but a relatively rare occurrence.
- The incidence of acute aortic dissection after AVR is thought to be 0.6% or less.
- Aortic size is generally accepted as an important risk factor, especially when it exceeds 6 cm.
- Look for annuloaortic ectasia after a previous AVR, especially when systemic hypertension is present.
- All patients known to have a mildly enlarged aorta after an AVR should have an echocardiogram at least every 6 months and should be reoperated electively once an increase in aortic diameter of > 50 mm becomes apparent.
- There are several ways of dealing with an enlarged aorta: by remodelling the aorta, using a supracoronary graft, or with a valved conduit.
Dr. Deepti H.V,
Senior Consultant Radiologist,
MHRG
Dr. Kamesh G,
Consultant Radiologist,
MHRG
Dr. C. Vaishali Raj,
Cross Section Fellow,
MHRG
