
A 18 year old male, History of headache since 1 month. Change of voice since 1 month.
FINDINGS
- MRI BRAIN WITH IV CONTRAST AND CORRELATIVE CT
A. LEGENDS
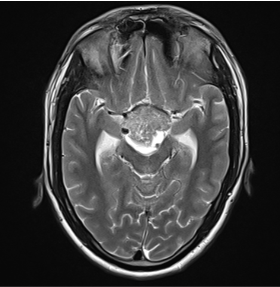
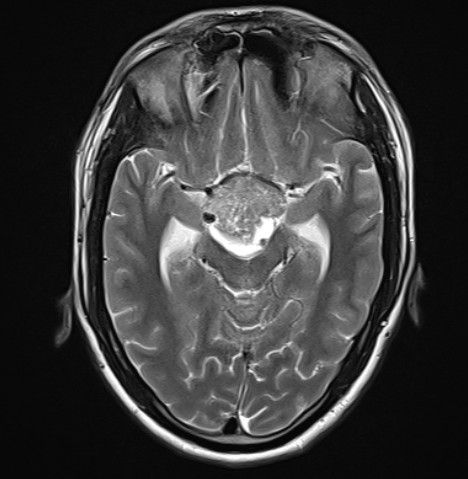
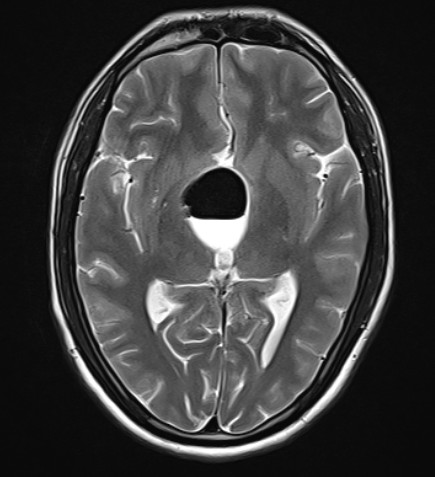
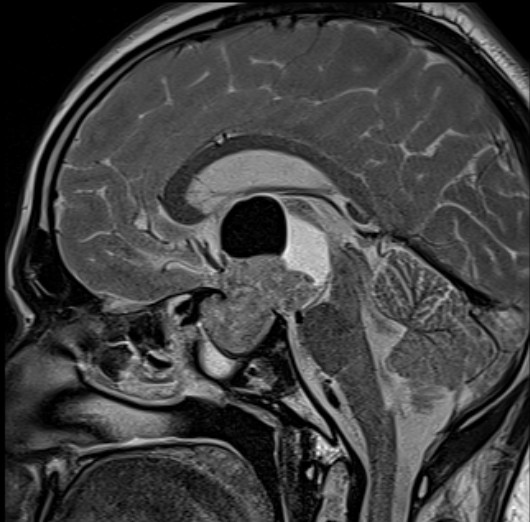
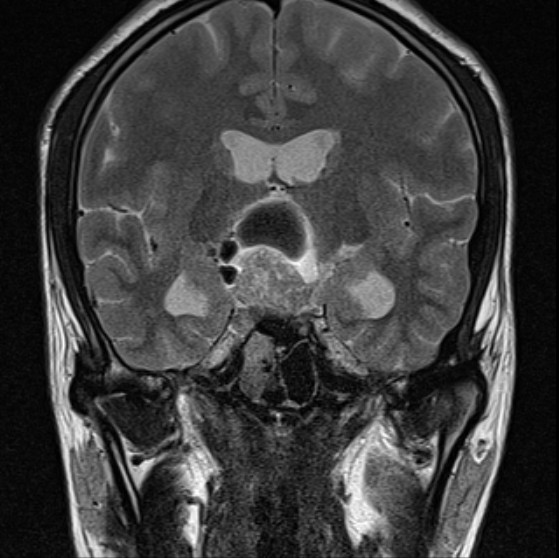
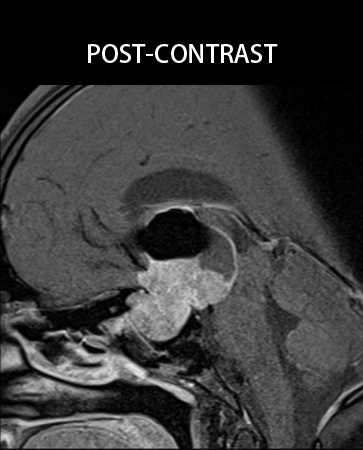
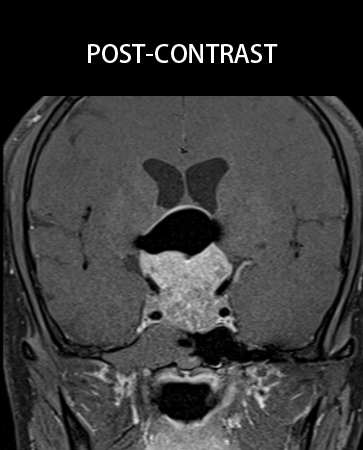
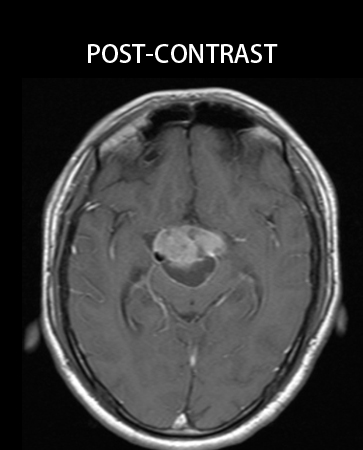
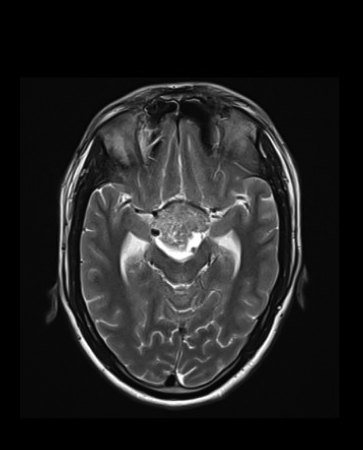
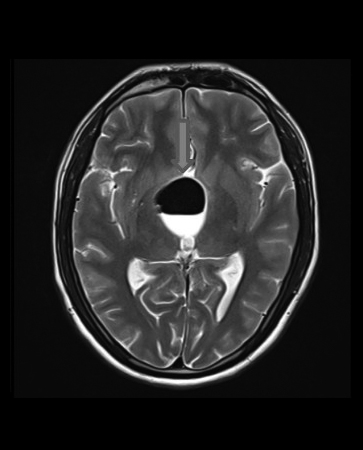
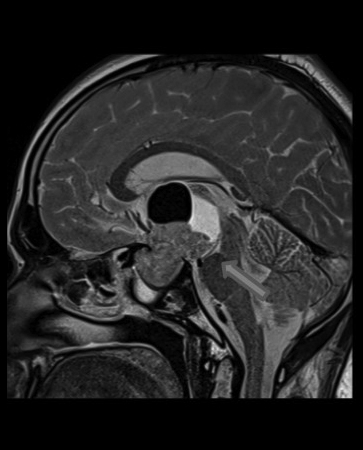
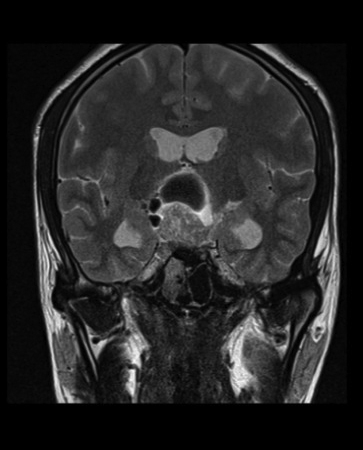
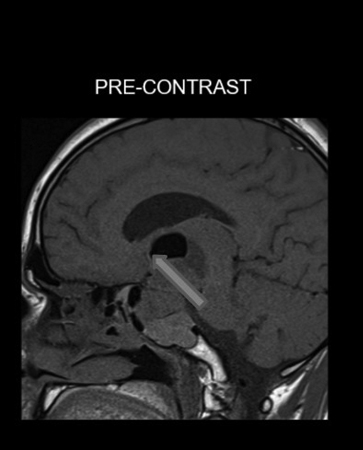
- A lobulated lesion seen in sellar – suprasellar region. The lesion predominantly T2 heterogeneous hyperintensity. Prominent cystic portion seen in the superior aspect of the lesion showing a prominent air – fluid level is seen.
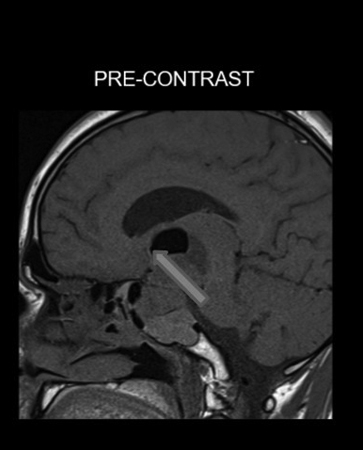
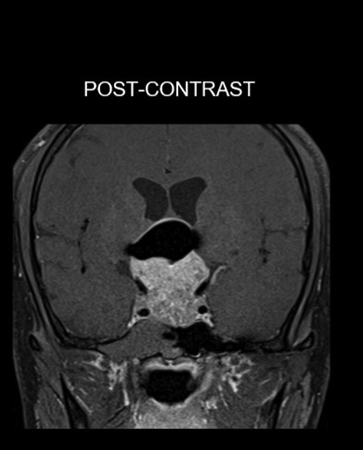
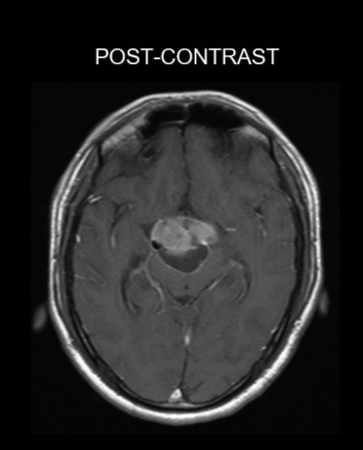
- The lesion predominantly shows T1 isointensity with significant heterogeneous contrast enhancement. Inferiorly, there is extension of the enhancing lesion into sphenoid sinus predominantly on the right. Pituitary gland not visualized separately.
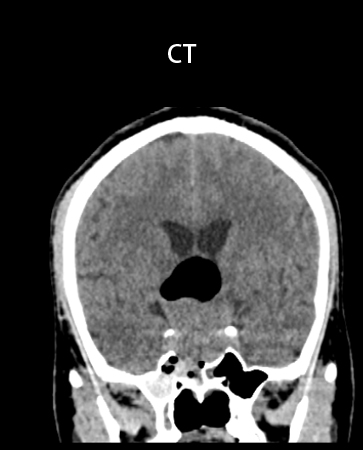
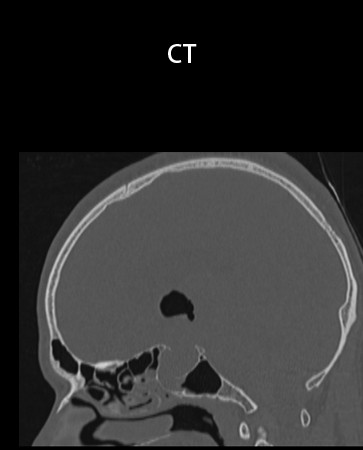
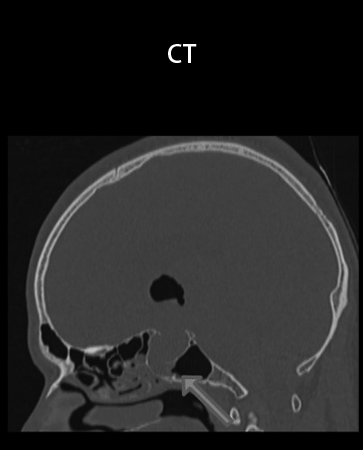
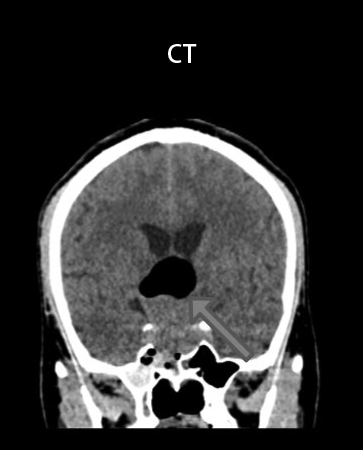
- Correlative CT shows marked widening of the sella with thinning of the walls, predominantly along the floor which shows areas of bony defects and rarefaction. Severe thinning and erosion of the roof of sphenoid sinus. No intralesional calcification.
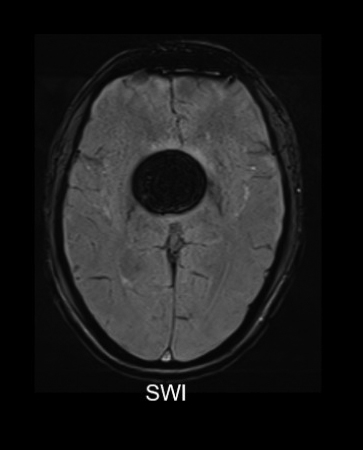
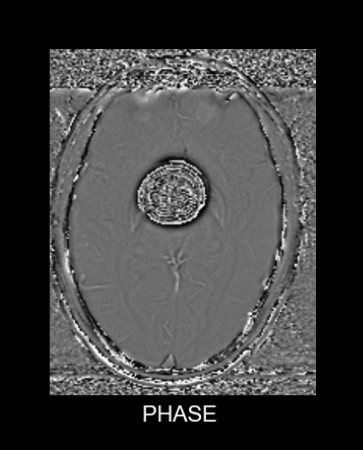
- Few T1 hyperintense, T2 isointense, hyperdense contents are seen in the body, lateral recess of sphenoid sinus and pneumatized pterygoid bone – likely represent hemorrhagic contents.
Diagnosis:
- Pituitary macroadenoma with intratumoral air fluid levels seen due to involvement of the sphenoid sinus.
Diagnosis:
- Pituitary adenomas are among the most common neurosurgical tumor. Macroadenomas are defined by their size, with a minimum diameter of 1 cm in the greatest dimension.
- Tumors are generally known to follow a path of least resistance, and as they grow, pituitary macroadenomas may extend to structures surrounding the sella turcica, including the sphenoid sinus, cavernous sinuses, or suprasellar region.
- Suprasellar extension of pituitary macroadenomas frequently occurs.It is hypothesized that anatomical variants of the sphenoid sinus may predispose to extrasellar growth of macroadenomas.
- Ectopic pituitary adenomas are defined as pituitary adenomas with no connection with normal pituitary gland. These , located in sphenoid sinus region are extremely uncommon.They may arise from the embryonal remnant of the extrasellar pituitary tissue in the sphenoid sinus or nasopharyngeal regions during the migration process of Rathke's pouch. These must not be confused with pituitary adenomas with sellar extension, as is our case.
- Macroadenomas are usually isointense with cortex.
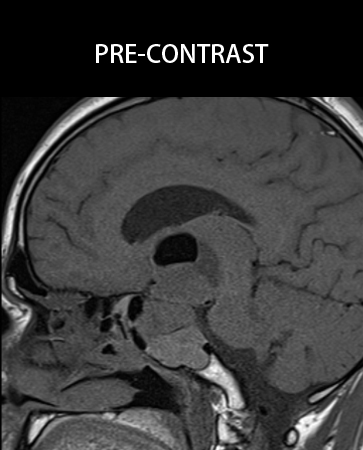
- The posterior pituitary "bright spot" is absent or displaced into the supradiaphragmatic cistern on T1-weighted sagittal scans.
- Small cysts and hemorrhagic foci are common. Fluid-fluid levels can be present but are more common in patients with pituitary apoplexy.
- Adenomas are generally isointense with gray matter on T2WI but can also demonstrate heterogeneous signal intensity.
- Hyperintensity along the optic pathways on T2/FLAIR can occur, in which macroadenomas compress the optic chiasm.
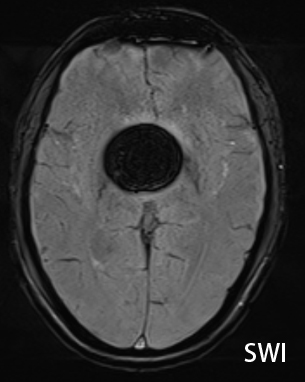
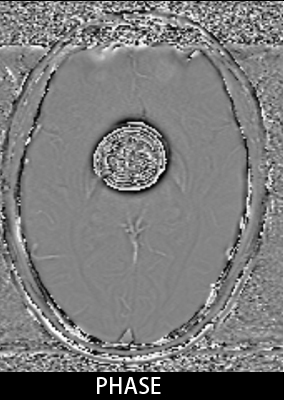
- Hemorrhagic adenomas "bloom" on T2*. Most macroadenomas enhance strongly but heterogeneously on T1 C+.
- Bone CT may show an enlarged, remodeled sella turcica. The lamina dura of the sellar floor is generally intact. However, "giant" pituitary adenomas may erode and extensively invade the skull base.
Management:
- Transsphenoidal resection of pituitary tumor.
References:
Sphenoid sinus anatomy and suprasellar extension of
pituitary tumors:Clinical article
DOI link: https://doi.org/10.3171/2013.3.JNS122113
Ectopic Sphenoid Sinus Pituitary Adenoma (ESSPA) with Normal Anterior Pituitary Gland: A Clinicopathologic and Immunophenotypic Study of 32 Cases with a Comprehensive Review of the English Literature
DOI link: link.springer.com/article/10.1007/s12105-012-0336-9
Osborn’s Brain -Imaging, Pathology and Anatomy
Dr. SHWETHA C
Junior Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr. NIKITHA U N
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
