

A 62 year old female, history of fever and abdominal pain.
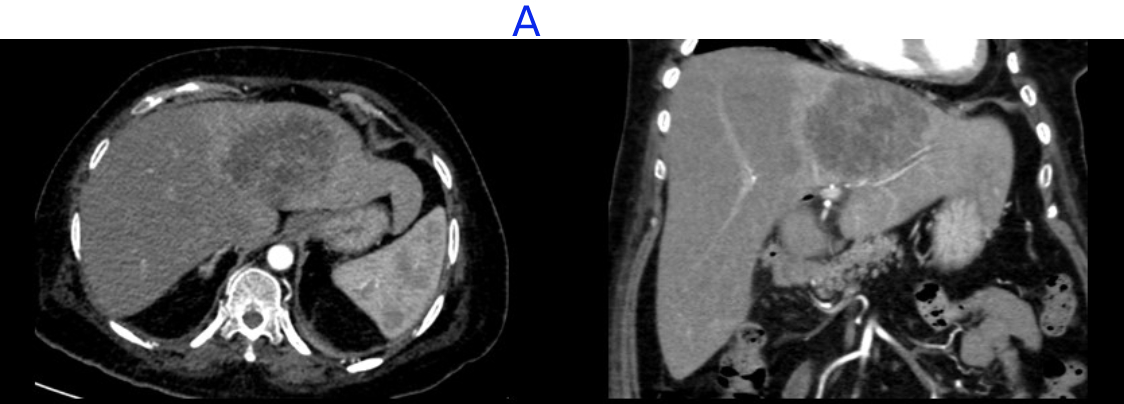
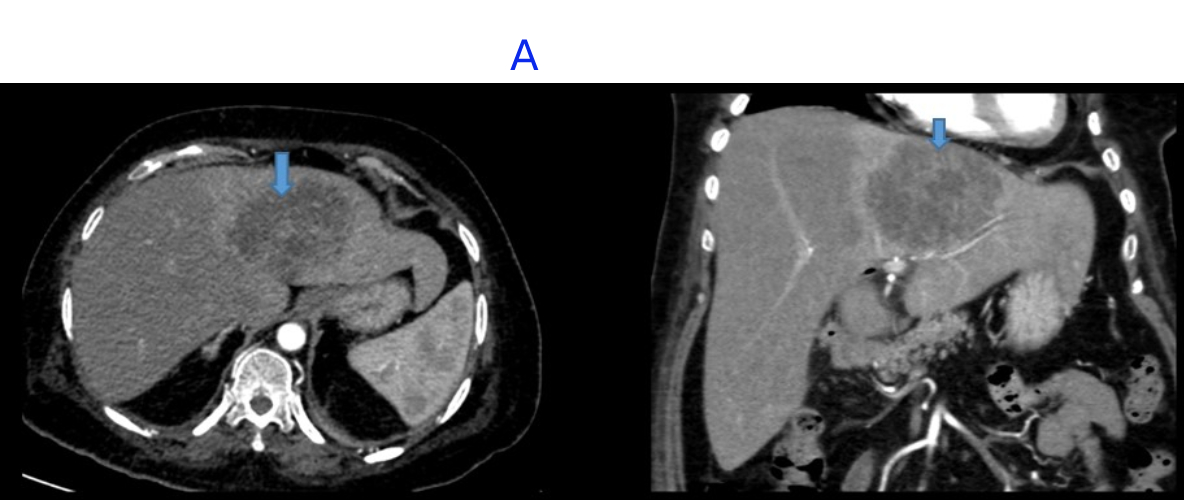
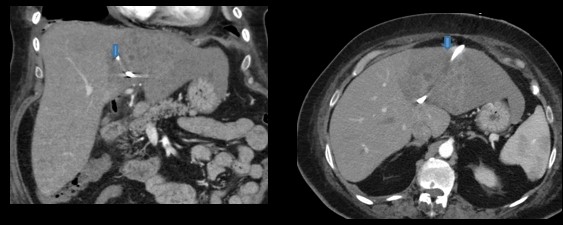
A. FINDINGS – CECT ABDOMEN AND PELVIS
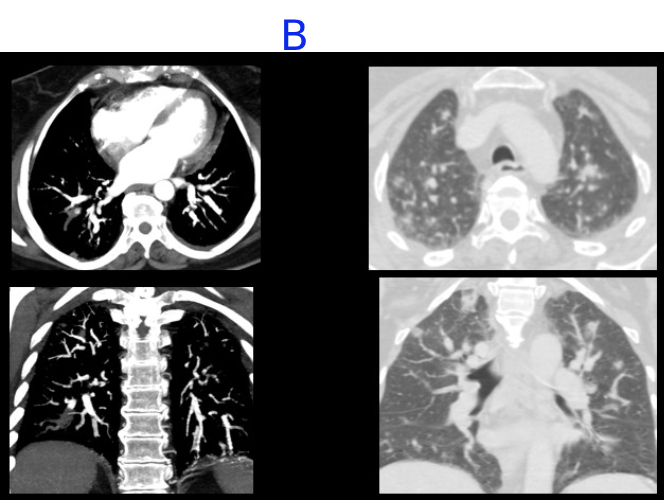
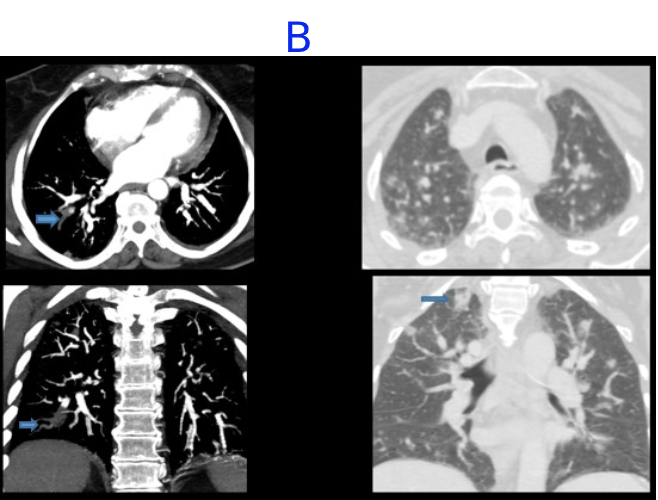
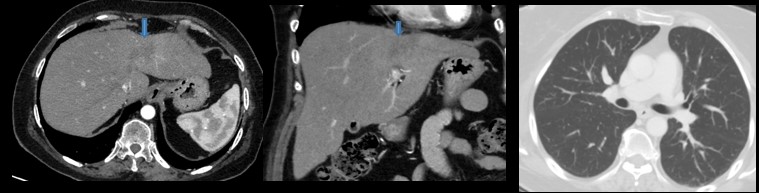
B. FINDINGS – CT PULMONARY ANGIOGRAPHY AND LUNG WINDOW
A. LEGENDS:
- Heterogeneous enhancing mass in the segment II and IVA of left lobe of liver with no venous washout.
B. LEGENDS:
- Acute thrombus in right lower lobe laterobasal segmental and subsegmental pulmonary artery.
- Multiple nodular ground glass opacities noted scattered in both lungs, some showing cavitation
DIFFERENTIAL DIAGNOSIS:
- Hepatic abscess and septic emboli in lungs.
- Neoplastic process; hepatic primary/ secondary with lung metastases.
- USG guided pig tail insertion was performed.
- HPE report: consistent with an abscess.
USG guided pig tail insertion was performed.Follow up after course of antibiotics, after 3 months
- Near complete resolution of heterogeneously enhancing lesion in left lobe of liver.
- Resolution of cavitating lung nodules.
DISCUSSION:
- Septic pulmonary embolism caused by liver abscess is rare but can cause considerable morbidity and mortality.
- Septic pulmonary embolism (SPE) is a type of non-thrombotic pulmonary embolism in which a thrombus containing microorganisms causes an inflammatory reaction.
- SPE thrombi can cause pulmonary infarction and metastatic abscesses.
- As complications of liver abscesses due to high rates of bacteremia, patients can sometimes develop pulmonary septic embolism, caused by clot, fibrin matrix and micro-organisms. Other complications include right sided endocarditis, pelvis thrombophlebitis.
- The main features on CT scan on septic pulmonary emboli is feeding vessel sign(79%), nodules with or without cavitations (79%) and subpleural wedge shaped subpleural opacities (64%).
- Liver abscess was the most frequently observed primary source of infection in SPE caused by K. pneumonia. Sometime are also associated with staphylococcus aureus and E.coli.
Management:
- Drainage of abscess guided by either CT or ultrasound, ERCP, followed by appropriate duration of the antibiotics. If the location is difficult to be accessed, open surgical drainage, laparoscopic drainage should be indicated.
- Antibiotics therapy should be continued for two to 4 weeks for complete drainage and 4 to 6 weeks for the incomplete drainage.
REFERENCES:
Chou DW, Wu SL, Chung KM, Han SC. Septic pulmonary embolism caused by a Klebsiella pneumoniae liver abscess: clinical characteristics, imaging findings, and clinical courses. Clinics (Sao Paulo). 2015 Jun;70(6):400-7. doi: 10.6061/clinics/2015(06)03. Epub 2015 Jun 1. PMID: 26106957; PMCID: PMC4462570.
Wang Y, Wang H, Liu Z, Chang Z. The Incidence of Septic Pulmonary Embolism in Patients with Klebsiella pneumoniae Liver Abscess: A Systematic Review and Meta-analysis. Gastroenterol Res Pract. 2022 Apr 15;2022:3777122. doi: 10.1155/2022/3777122. PMID: 35462985; PMCID: PMC9033355.
Seo, Dong Joo MD1; Bains, Kanwal MD1; Aslam, Aysha MD2. S3519 Septic Pulmonary Emboli From Pyogenic Liver Abscess After Cholecystectomy. The American Journal of Gastroenterology 115():p S9, October 2020. | DOI: 10.14309/01.ajg.0000716124.94675.1e
Dr RAJESH HELAVER
Senior Consultant Radiologist
MHRG
Dr NEHA SATHYANARAYANA
Radiology Resident
MHRG
