
75y old male presented with numbness in right upper limb since 1 day associated with slurring of speech
Clinical features :
- 75y old male presented with numbness in right upper limb since 1 day associated with slurring of speech.
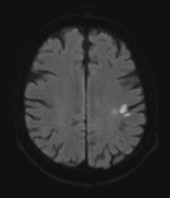
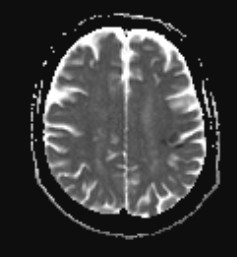

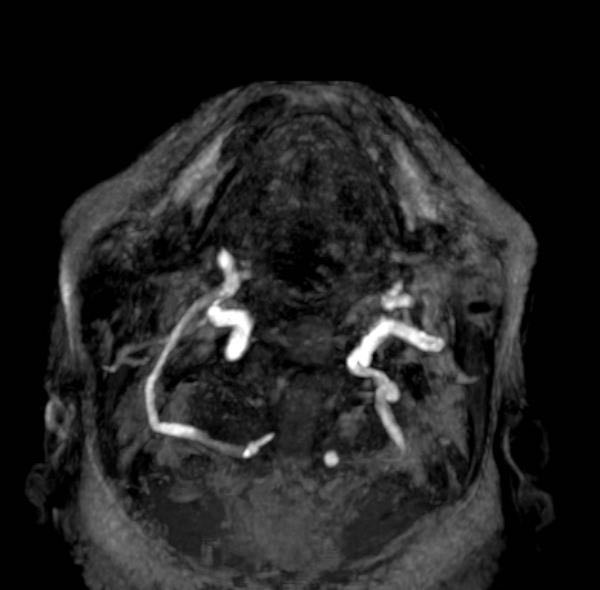

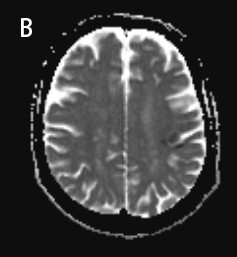
- Acute infarct showing diffusion restricting (Green arrow) in left perirolandic region. Axial MIP image (Figure C) showing no significant narrowing in circle of Willis
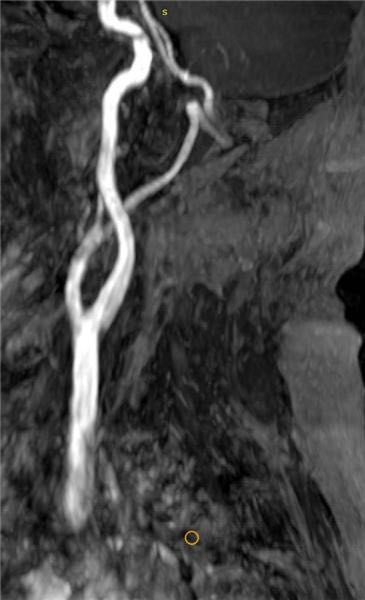
- Oblique reformatted images (Fig A, B and C) showing normal left vertebral artery and absent V1, V2 and V3 segments of right vertebral artery (Yellow arrow, Fig A). V4 segment of the right vertebral artery seen arising from external carotid artery, coursing through the foramen magnum (Blue arrow, Fib B,C).





Diagnosis:
- Type II persistent right Proatlantal artery (carotid-vertebrobasilar anastomose.
Introduction:
- In the early phase of embryonic development, the blood supply to the posterior fossa is entirely dependent on the anterior circulation through carotid-vertebrobasilar anastomoses, these include trigeminal artery, the otic artery, the hypoglossal artery, and the ProA.
- The otic artery is the first vessel to obliterate, followed by the hypoglossal, trigeminal, and ProA arteries (1).
- Persistent carotid-vertebrobasilar anastomoses are rare, with an overall prevalence of 0.1% to 1.0%. The incidence rate of persistent carotid-vertebrobasilar anastomoses is inversely related to the order of regression. The trigeminal is the most common, followed by the hypoglossal, otic, and ProA arteries (3).
Discussion:
The proatlantal artery is one of the persistent carotid - vertebrobasillar anastomoses.
- There are two types, depending on its origin:
- Type I: (~55%)
- Arises from the internal carotid artery.
- type II: (~40%)
- Corresponds to the second segmental artery
- Arises from the external carotid artery.
- Rarely it arises from the common carotid artery (2).
- Irrespective of their origin, the artery passes through the foramen magnum and joins the vertebral artery.
Imaging differential:
- The hypoglossal and ProA are similar but can be differentiated by their course and skull entry site.
- The hypoglossal course can have a higher origin at the C1 vertebra or the C1 to C2 interspace, is vertically oriented, and enters the skull through the hypoglossal canal.
- In contrast, the ProA typically arises from the C2 or C3 vertebral level, has a suboccipital horizontal course similar to the V3 segment, and enters the skull through the foramen magnum.
- Proximal VAs are absent or hypoplastic in half of the individual with persistent ProA.
Prognosis
- Variants are commonly associated with other vascular anomalies such as vertebral artery aplasia or hypoplasia and have an increased incidence of intracranial aneurysm formation.
- Although patients with proatlantal arteries are generally asymptomatic, they remain at increased risk of posterior circulation hemorrhage secondary to altered hemodynamics, as well as ischemia in the setting of occlusion of these variant arteries.
Reference
- Raybaud C. Normal and abnormal embryology and development of the intracranial vascular system. Neurosurg Clin N Am. 2010;21:399–426.
- Choudhary G, Ahuja K, Khan R, Kubal W. Bilateral persistent primitive hypoglossal artery presenting with hemiplegia. J Radiol Case Rep. 2018;13(5):1072–1075. doi: 10.1016/j.radcr.2018.04.022.
- Yilmaz E, Ilgit E, Taner D. Primitive persistent carotid-basilar and carotid-vertebral anastomoses: a report of seven gases and a review of the literature. Clin Anat. 1995;8(1):36–43. doi: 10.1002/ca.980080107.
Dr Sriram Patwari
MBBS, MD, PDCC, EDiNR
Senior Consultant Manipal Hospitals Radiology Group.
Dr Sanjana.N
MBBS, M.D.
Cross section imaging fellow - MHRG.
