

22 years old with insidious onset distal forearm and hand weakness (right>left)
22 years old with insidious onset distal forearm and hand weakness (right>left)

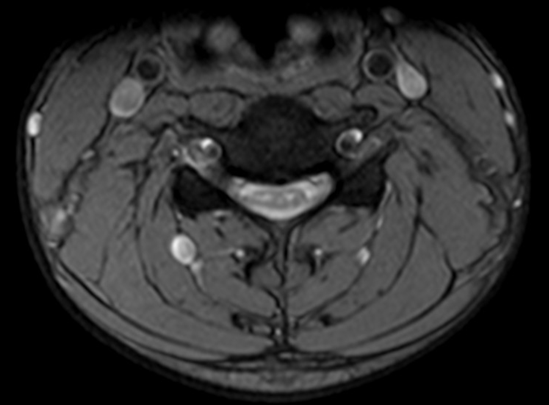



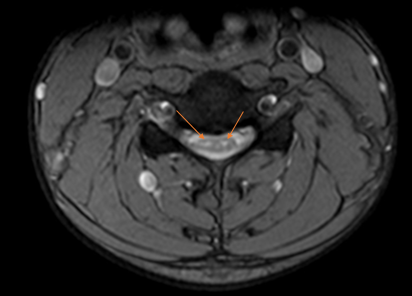
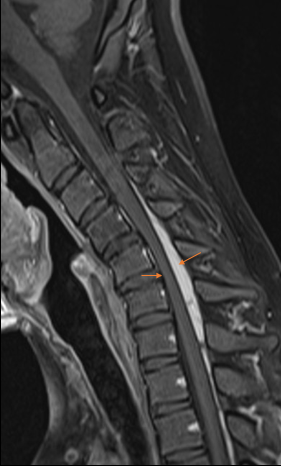
T2?weighted sagittal MRI in a neutral position (Fig 1) and in neck flexion (Fig 3) shows anterior displacement of the posterior dura (blue arrow in Fig 3) with resultant anterior displaced cord indenting the posterior vertebral margin with associated thinning of the spinal cord and myelomalacia. Epidural flow voids seen posterior to the dura are also seen (Orange arrow in Fig 3). There is bilateral grey horn cell hyperintensity resembling owls' eye appearance on the axial GRE image (Fig 2). The T1?weighted post-contrast flexion (Fig 5) MRI reveals enhancement in the posterior epidural space (orange arrow in Fig 5) suggestive of engorged posterior epidural venous plexus.



Diagnosis:
Hirayama Disease
Discussion:
- Hirayama disease is a rare condition characterized by asymmetric distal muscle weakness and atrophy in young adults. Commonly affects men in 2nd to 3rd decades. The disease is more prevalent in India, Japan, and other Asian countries.
- The disease is attributed to forward displacement of the posterior lower cervical dura when the neck is in flexion causing dynamic cord compression. The pathomechanism is debated, but the prevailing theory postulates that insufficient growth of the dura relative to the spinal column during puberty allows forward displacement of the dura in flexion with compression of the spinal cord, possibly leading to ischemia of the anterior horn cells at C8 and T1
- Clinically patients present with insidious onset of unilateral upper extremity weakness involving the distal forearm and hand muscles, rarely asymmetric bilateral involvement. No sensory disturbances/autonomic disturbances/pyramidal signs are seen.
- Conventional neutral position MR imaging may show thinned lower cervical cord and asymmetric cervical cord flattening with or without abnormal T2-weighted hyperintensities in the cervical cord, especially the anterior horn cells. Owls' eye appearance of anterior grey horn degeneration can also be seen.
- MR imaging with neck flexion, reveals classic findings of forward shifting of the posterior dural sac and loss of attachment between the posterior dural sac and the subjacent lamina with engorged posterior epidural venous plexus showing uniform enhancement on post-contrast images.
- Imaging pearl: Always consider dynamic contrast MRI of the cervical spine with neutral / flexion views if lower cervical cord atrophy/myelomalacia without evident cause in a young patient with insidious onset asymmetric upper limb weakness.
Dr. Sriram Patwari
MD, PDCC (Neuroradiology)
Consultant Radiology, Co-lead Neuroradiology
Manipal Hospitals Radiology Group
Dr C. Chavadi
DMRD, DNB
Senior Consultant Radiology
Manipal Hospitals Radiology Group

