
A 76-year gentleman with post resection of sigmoid malignancy and descending colostomy. Now complains of abdominal discomfort and low stoma output.
A 76-year gentleman with post resection of sigmoid malignancy and descending colostomy. Now complains of abdominal discomfort and low stoma output.

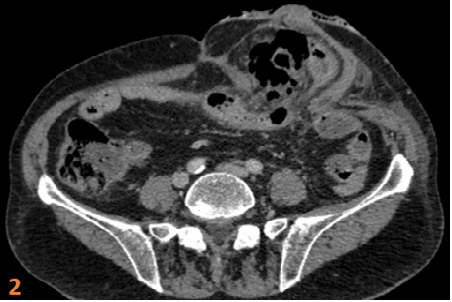
- Herniation of jejunal loops and omentum through the stomal defect (arrow) with minimal free fluid (star) within the hernial sac (Fig 1).
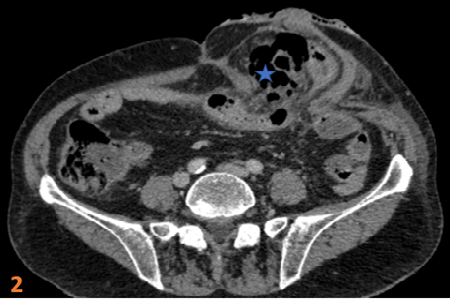
- Presence of air in the herniated sac (star) (Fig 2).
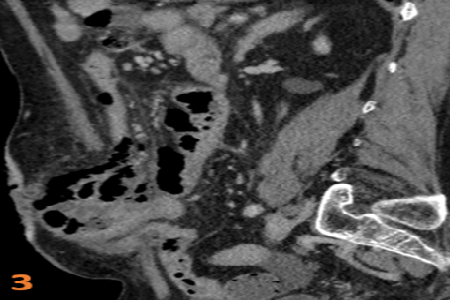
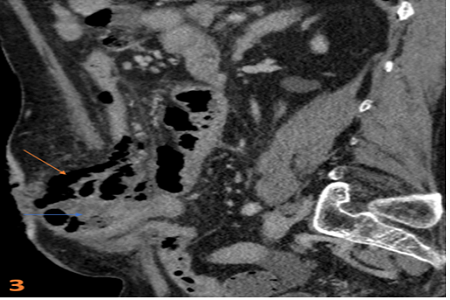
- Air in the herniated sac tracking along the small bowel mesentery (orange arrow). Suspicious hypo enhancement of herniated jejunal loops with mild circumferential wall thickening (blue arrow) (Fig 3).
- All these findings were in favour of jejunal perforation, but it was surgically proven to be jejunal diverticulitis without perforation.

DIAGNOSIS:
Jejunal diverticulitis in a parastomal hernia masquerading as perforation.
DISCUSSION:
- Small-bowel diverticula are detected on barium studies in about 2% of patients. This condition is known as jejunoileal diverticulosis or simply jejunal diverticulosis because most of the diverticula are located in the jejunum.
- Jejunal diverticulosis is important because it is associated with a variety of complications, including stasis and bacterial overgrowth, diarrhea, malabsorption, intestinal pseudo-obstruction, gastrointestinal bleeding, diverticulitis, and, rarely, free perforation with peritonitis.
- Jejunal diverticulosis is readily diagnosed on barium studies of the small bowel by the presence of multiple rounded, variably sized jejunal outpouchings, often seen in profile to have discrete, relatively narrow necks.
- At computer tomography small bowel diverticulitis usually presents as a focal area of bowel wall thickening most prominent on the mesenteric side of the bowel with adjacent inflammation and/or abscess formation.
- When an abscess is present, CT findings may include relatively smooth margins, areas of low attenuation within the mass, rim enhancement after IV contrast administration, gas within the mass, displacement of the surrounding structures, and edema of thickening of the surrounding fat or fascial planes.
DIFFERENTIAL DIAGNOSIS:
Strangulated hernia with ischemia and perforation of jejunal loops (due to hypo enhancement of herniated jejunal loops with mild free fluid and air in herniated sac tracking along small bowel mesentery).
REFERENCES:
- Fintelmann F, Levine MS, Rubesin SE. Jejunal diverticulosis: findings on CT in 28 patients. American journal of roentgenology. 2008 May;190(5):1286-90.
- De Peuter B, Box I, Vanheste R, Dymarkowski S. Small-bowel diverticulosis: imaging findings and review of three cases. Gastroenterology research and practice. 2009 Jan 1;2009.
Dr. Pravin Kumar M DMRD,DNB
Senior Consultant – Radiology
Columbia Asia Hospital, Hebbal.
Dr Vivek Jirankali MD,
Senior Resident and Cross-sectional fellow
Columbia Asia Radiology Group.
