
39 year old female patient presented with shortness of breath with history of persistent cough since 3 weeks and intermittent fever. No weight loss.
- 39 year old female patient presented with shortness of breath with history of persistent cough since 3 weeks and intermittent fever. No weight loss.
- On clinical examination, SPO2: 88% with reduced air entry in the right hemithorax.
- Xray and CT thorax were performed.
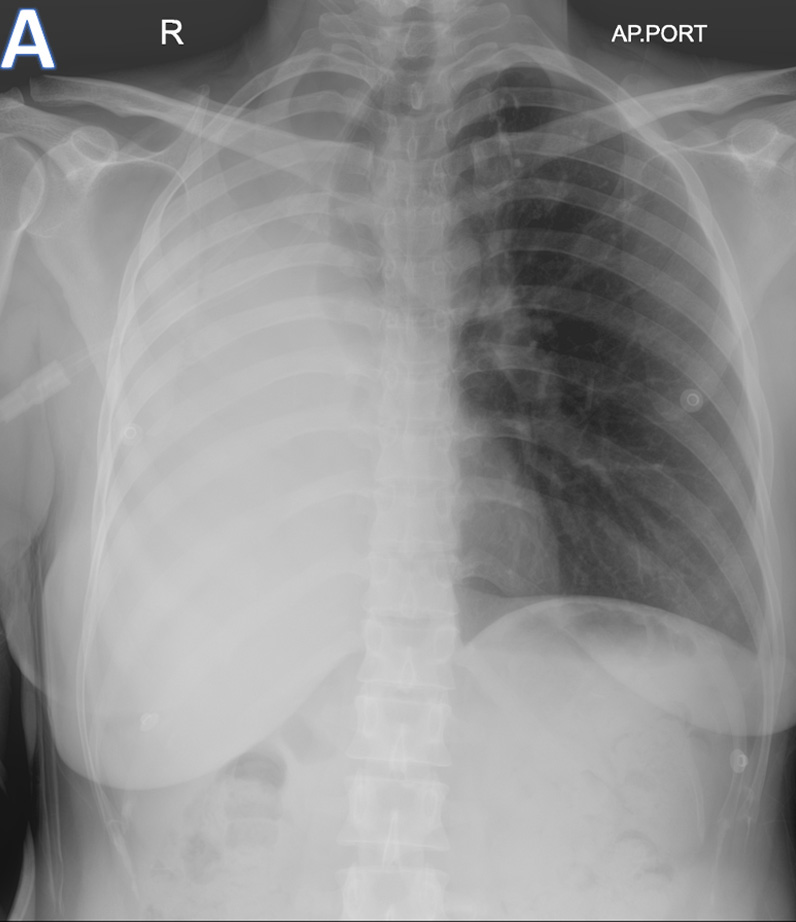


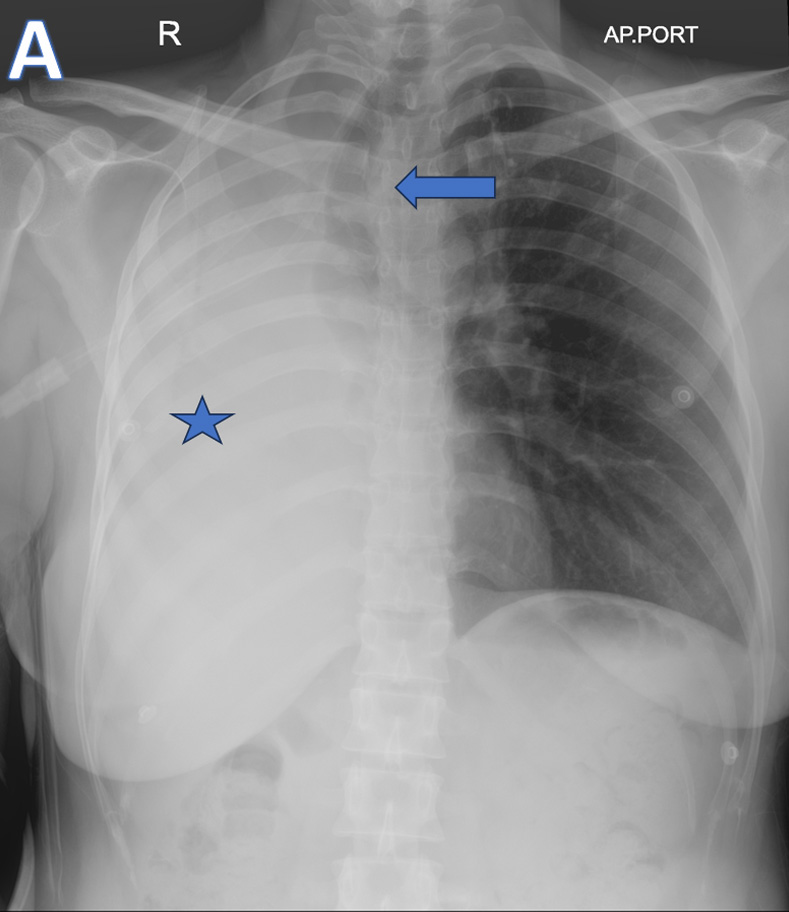
A - AP-Chest XRAY
- ARROW: Tracheal deviation to the Right.
- STAR: Opacified right hemithorax.
- Findings are consistent with Collapse of the right lung.
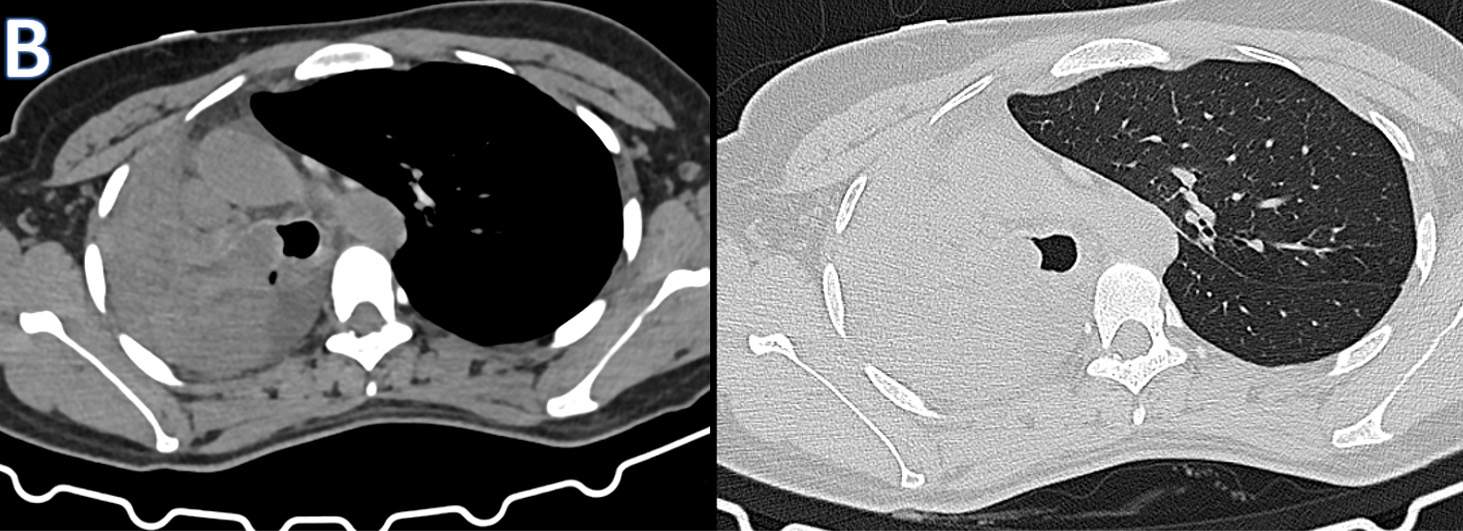
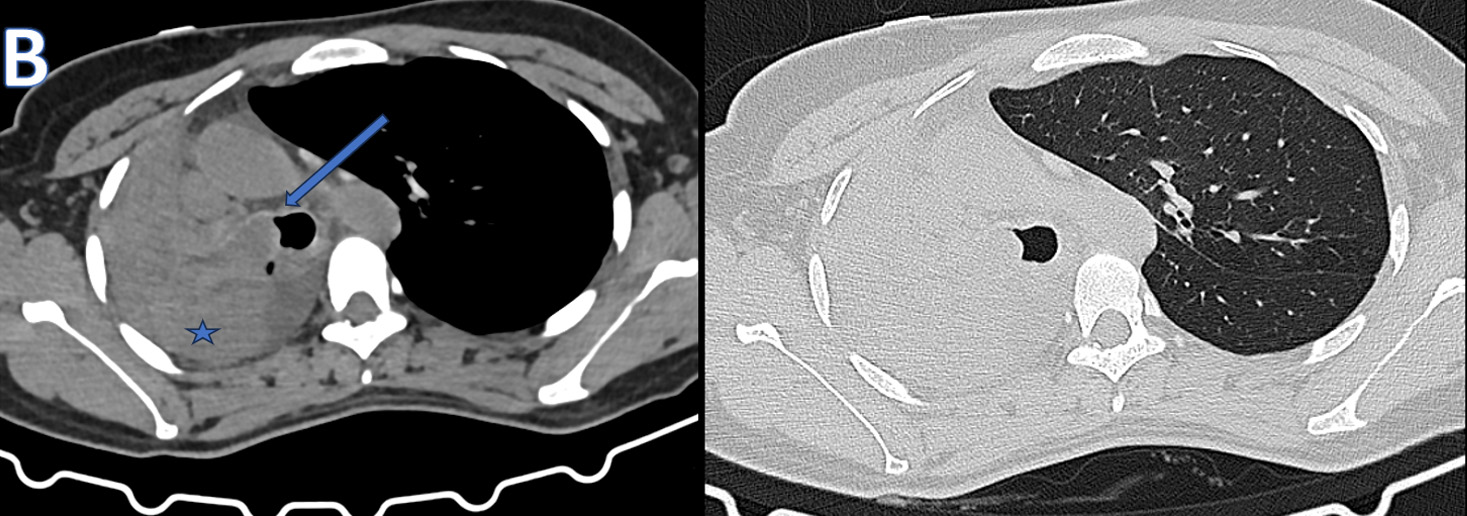
B – Axial CT thorax (soft tissue and lung window images)
- ARROW: Soft tissue density endobronchial mass lesion in the right main bronchus.
- STAR: Collapsed right lung and hypodense fluid in the right hemithorax.
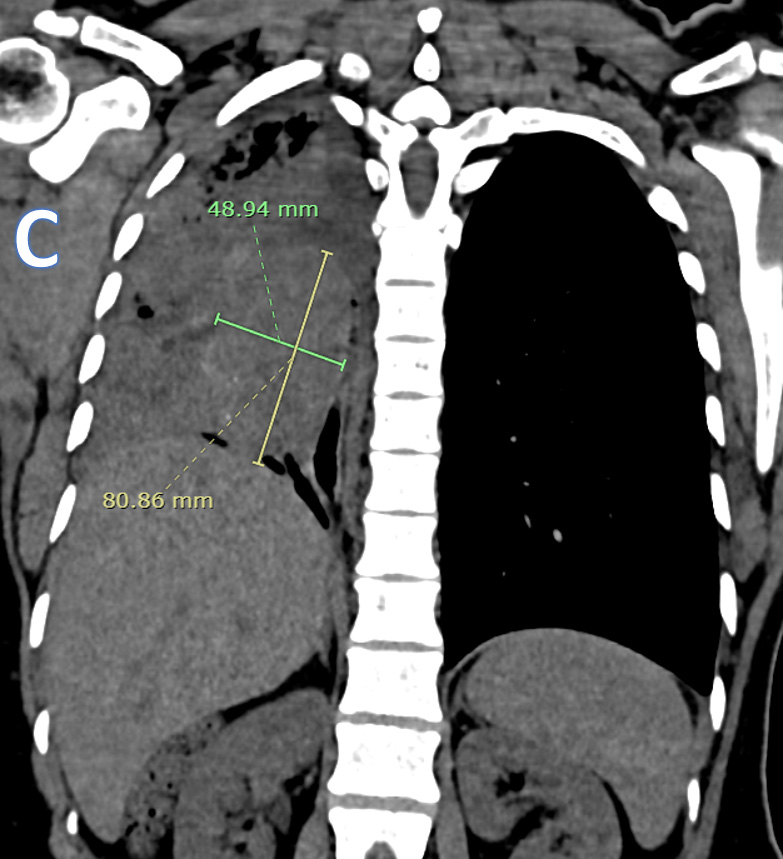
C – CORONAL CT THORAX
Ovoid heterogeneously isodense mass lesion with multiple tiny peripheral specks of calcifications in the right hemithorax with endobronchial extension.
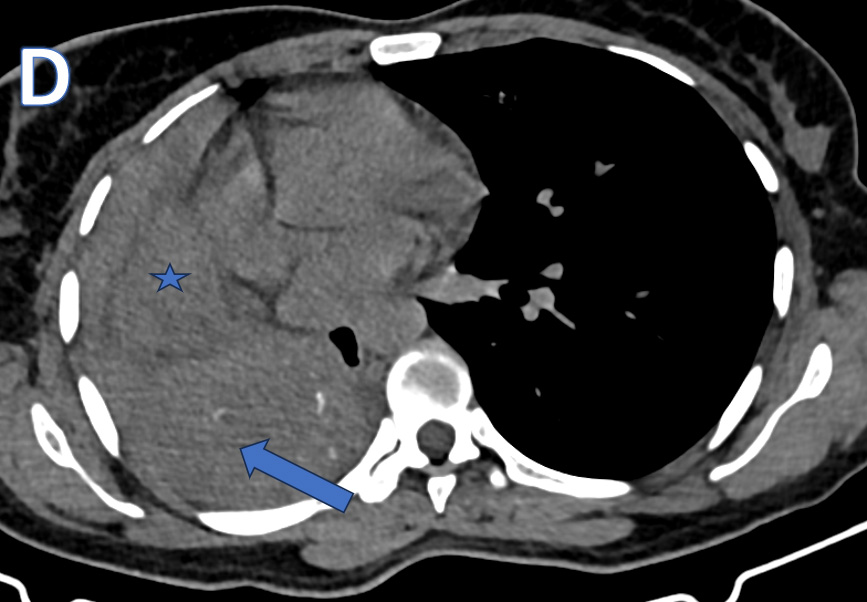
D – Axial CT Thorax
- ARROW: Isodense mass lesion with peripheral calcific specks and endobronchial extension.
- STAR: Organised / Clotted - Hemorrhagic contents in the right hemithorax.
FINDINGS AND IMPRESSION
- Ill-defined soft tissue density mass with few peripheral calcific specks in the right hemithorax extending into the right main bronchus with resultant bronchus cut off.
- Associated near complete collapse of the right lung with ipsilateral tracheo mediastinal shift.
- Irregular soft tissue density foci scattered within the right thoracic cavity with mild to moderate fluid – suggestive of haemothorax with organized haemorrhagic products.
- Mediastinal lymphadenopathy.
IMPRESSION: Centrally obstructing right hemithroacic endobronchial mass – likely neoplastic in etiology.
- DDX:
- Endobronchial malignancy like Bronchial carcinoid and Primary lung carcinoma—rare but possible at this age.
- Less likely: Inflammatory endobronchial lesion or Endobronchial metastasis
Diagnosis
- Bronchoscopy –Right main bronchus completely occluded by mass.
- Biopsy – HPE: ATYPICAL CARCINOIDE TUMOR.
DISCUSSION - Endobronchial Carcinoid Tumor
- Neuroendocrine tumors arising from Kulchitsky cells of the bronchial mucosa
- Represent the most common primary endobronchial neoplasm in young adults
- Typically slow-growing but may cause significant airway obstruction
Histopathology
- Composed of uniform neuroendocrine cells arranged in nests, trabeculae, or rosettes.
- Classified as:
- Typical carcinoid: <2 mitoses/2 mm², no necrosis
- Atypical carcinoid: 2–10 mitoses/2 mm² and/or necrosis
Incidence and Epidemiology
- Account for 1–2% of all primary lung tumors.
- Incidence: ~0.2–2 cases per 100,000 population/year. Younger age group compared to other lung malignancies - Peak incidence: 30–50 years
- Slight female predominance. No strong association with smoking, especially for typical carcinoids.
Clinical Presentation
- Symptoms largely due to bronchial obstruction
- Dyspnea
- Recurrent pneumonia
- Hemoptysis (common due to tumor vascularity)
- Carcinoid syndrome is rare (<5%) in pulmonary carcinoids
- Delayed diagnosis common due to nonspecific symptoms
Radiological Findings
CHEST RADIOGRAPH
- Lobar or whole lung collapse
- Recurrent or non-resolving consolidation
- Opacified hemithorax with ipsilateral mediastinal shift in severe obstruction.
CT THORAX
- Well-defined central endobronchial mass
- Typically isodense to muscle
- Intense enhancement post-contrast (hypervascular)
- Secondary findings:
- Atelectasis
- Post-obstructive pneumonia
- Mucoid impaction
- Pleural effusion or hemorrhage (occasionally)
Other Diagnostic Imaging
- Contrast-enhanced CT: modality of choice for initial evaluation
- Somatostatin receptor imaging:
- ^68Ga-DOTATATE PET/CT shows high sensitivity
- Bronchoscopy:
- Direct visualization: smooth, cherry-red, highly vascular mass
- Biopsy with caution due to bleeding risk
Prognosis and Management
- Surgical resection is the treatment of choice
- Excellent prognosis:
- 5-year survival:
- Typical carcinoid: >90%
- Atypical carcinoid: 60–75%
- 5-year survival:
- Early radiologic diagnosis prevents irreversible lung damage
Imaging Diagnostic Pearls
- Central enhancing endobronchial mass in a young, non-smoker → think carcinoid
- Persistent lobar collapse or recurrent pneumonia in the same distribution is a red flag
- Marked enhancement helps distinguish carcinoid from mucus plug or foreign body
- Lack of nodal disease favors typical carcinoid
- Always evaluate for endobronchial extension on CT lung windows
References
- Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization classification of lung tumors. J Thorac Oncol. 2015;10(9):1243–1260.
- Caplin ME, Baudin E, Ferolla P, et al. Pulmonary neuroendocrine (carcinoid) tumors: ESMO Clinical Practice Guidelines. Ann Oncol. 2015;26 Suppl 5:v102–v108.
- Erasmus JJ, McAdams HP, Patz EF Jr, Goodman PC. Bronchial carcinoid tumors: radiologic findings in 22 patients. Radiology. 1998;206(2):497–502.
- Chong S, Lee KS, Chung MJ, et al. Neuroendocrine tumors of the lung: clinical, pathologic, and imaging findings. Radiographics. 2006;26(1):41–57.
- Kayser K, Zink S, André S, et al. Typical and atypical carcinoid tumors of the lung: differentiation by morphometry and immunohistochemistry. Pathol Res Pract. 2001;197(10):697–703.
DR. K VISHNU VARDHAN REDDY
MBBS, MD, Fellowship In Cross Section Imaging (MHRG).
