3 year 11 month old female child presenting with complaints of three episodes of seizures lasting for 1-5 minutes with no regain of consciousness in between.
A. FINDINGS: MRI BRAIN WITH IV CONTRAST
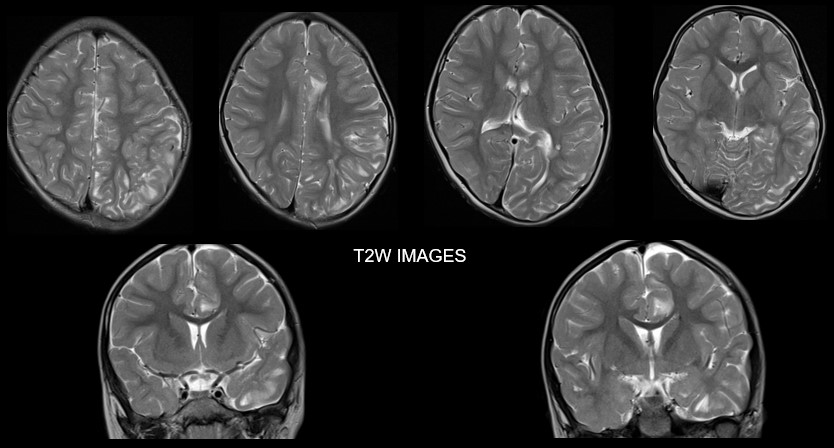
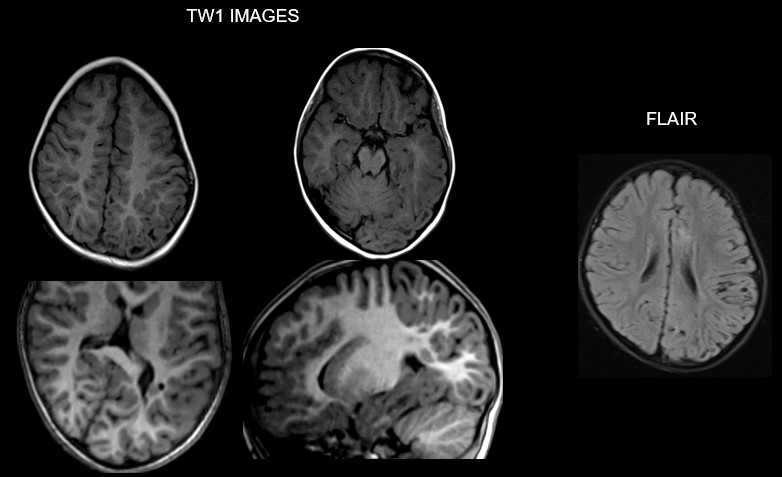
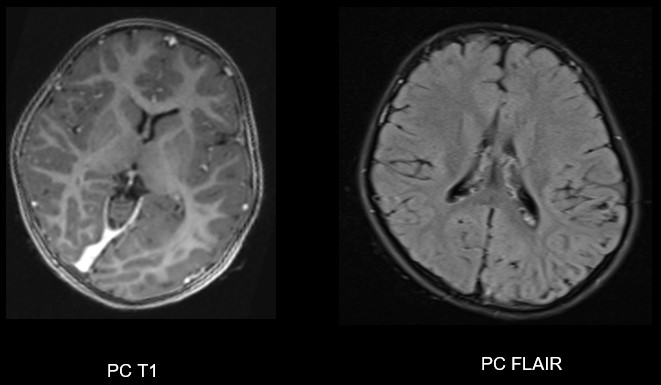
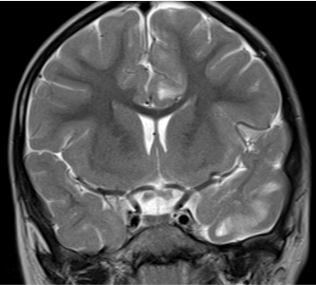
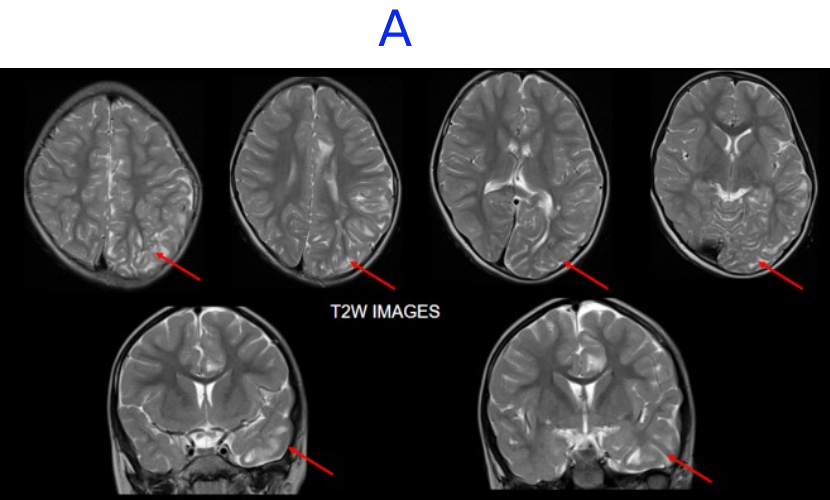
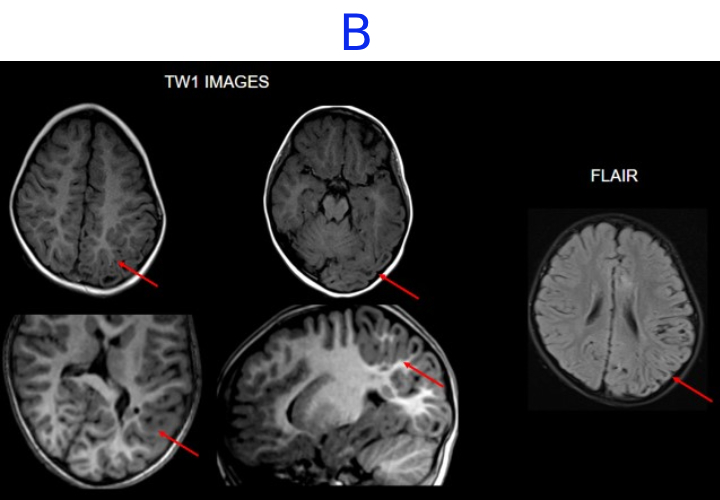
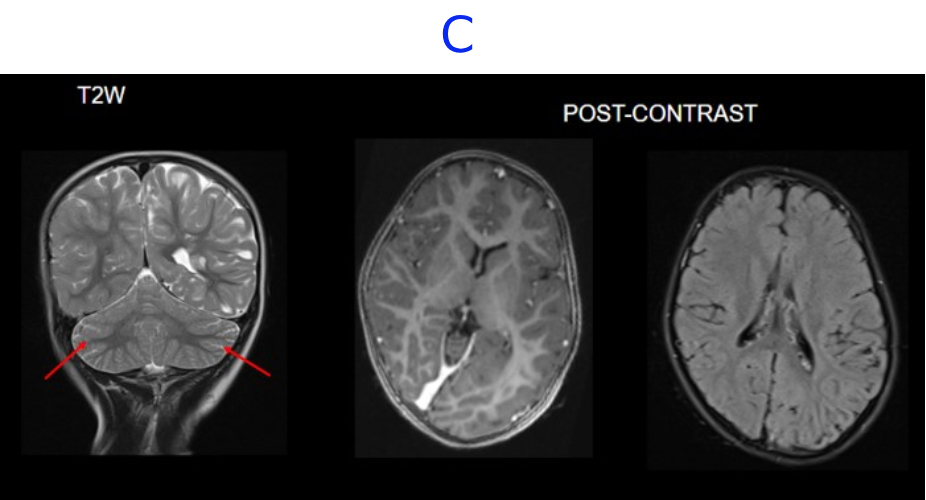
- A. There is hemihemimegelencephaly in the left parieto-temporo-occipital lobes, characterized by enlargement of the involved hemisphere. There is associated gyral thickening with white matter signal changes in the adjacent subcortical white matter.
- B. Areas of rarefaction are seen in white matter signal changes. Note is also made of periventricular nodular heterotropia along the atrium of the left lateral ventricle.
- C. No volume loss in bilateral cerebellar hemispheres. No abnormal post-contrast enhancement.
DIAGNOSIS:
Left posterior quadrantic dysplasia with associated subcortical white matter signal abnormalities and periventricular nodular heterotropia.
DISCUSSION:
- Hemimegalencephaly (HMEG) is defined as complete unilateral megalencephaly that affects one entire or almost an entire brain hemisphere.
- Focal megalencephaly, which involves up to three cerebral lobes, has been referred to as quadrantic dysplasia, lobar HMEG, or hemi-HMEG and typically affects the frontal lobe or the parieto-occipital lobes
- Posterior quadrantic dysplasia (PQD), also sometimes called hemi-hemimegalencephaly, is a rare disorder of cortical development that comprises 3–15% of cases of multilobar cortical dysplasia.
- PQD typically involves the temporal, parietal, and occipital lobes of one cerebral hemisphere (the posterior quadrant of the cerebrum) with sparing of the frontal lobe.
- Like hemimegalencephaly, PQD results from hamartomatous overgrowth of the involved parenchyma.
Clinical features:
- Seizures are the hallmark clinical presentation of PQD, and patients most commonly present with infantile spasms prior to 1 year of age.
- Additional symptoms common to PQD include intellectual disability, developmental delay, hemiparesis, and visual deficits.
- Disorders characterised by brain overgrowth spectrum viz megalencephaly, hemimegalencephaly and FCD type II are strongly associated with mutations in the mTOR pathway.
- The mechanistic target of rapamycin (mTOR) pathway is a critical regulator of cell growth, proliferation, and migration during brain development. Mutations in key genes within this pathway (e.g., MTOR, AKT3, PI3K, DEPDC5) lead to its hyperactivation, which is the underlying mechanism for the cellular overgrowth observed in these disorders.
- The link to the mTOR pathway is crucial because it opens opportunities for potential targeted therapies using mTOR inhibitors, which may regulate the pathway function and improve outcomes, though surgical resection remains the primary treatment for intractable epilepsy.
MANAGEMENT:
- Treatment of PQD centers around management of refractory epilepsy.
- If surgical management of epilepsy is required, less extensive and therefore less debilitating functional disconnective surgery is often possible with PQD in comparison with hemimegalencephaly and multilobar cortical dysplasias, given more localized cerebral involvement.
- Early intervention boasts high success rates, with seizure freedom reported in as many as 92% of pediatric cases.
Malformations of Cortical Development: Updated Imaging Review
Julia M Brunelli et al.
DOI-Link: https://doi.org/10.1148/rg.230239
Posterior Quadrantic Dysplasia
https://www.ajnr.org/ajnr-case-collections-diagnosis/posterior-quadrantic-dysplasia
Dr. Gauri Bornak
Associate Consultant Radiologist
Manipal Hospital Radiology Group
Dr. NIKITHA U N
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru