A 75 year old, with left 3rd and 6th nerve paresis. History of left herpes zoster.
A.FINDINGS
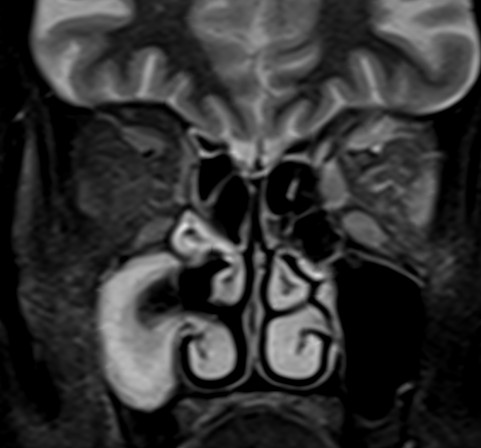
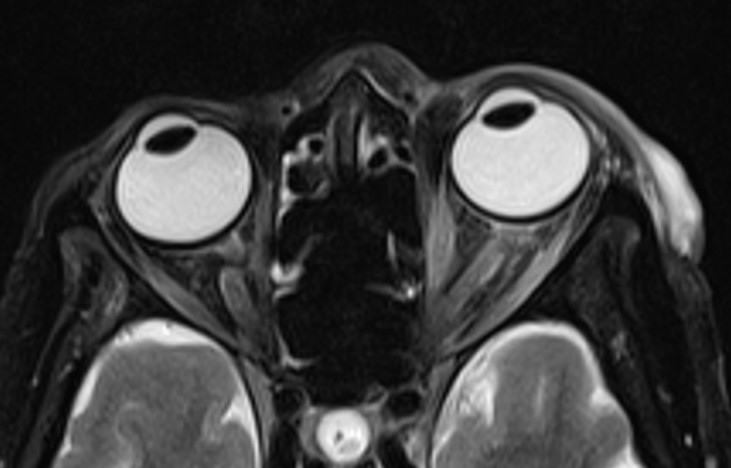
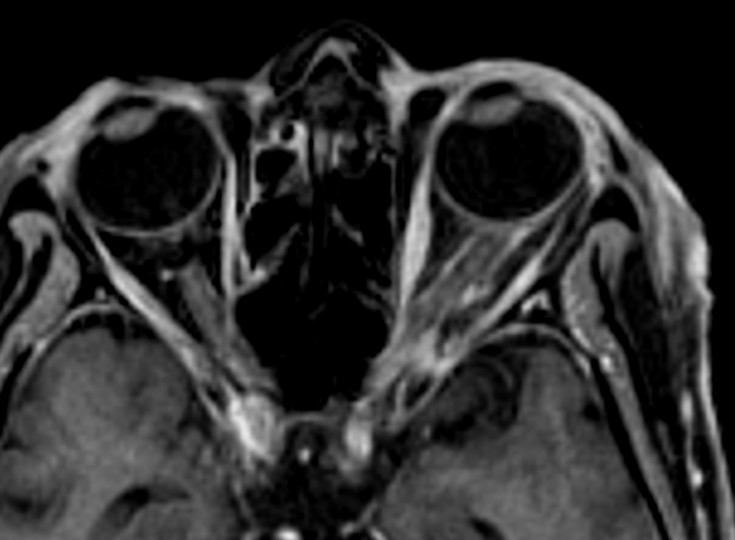
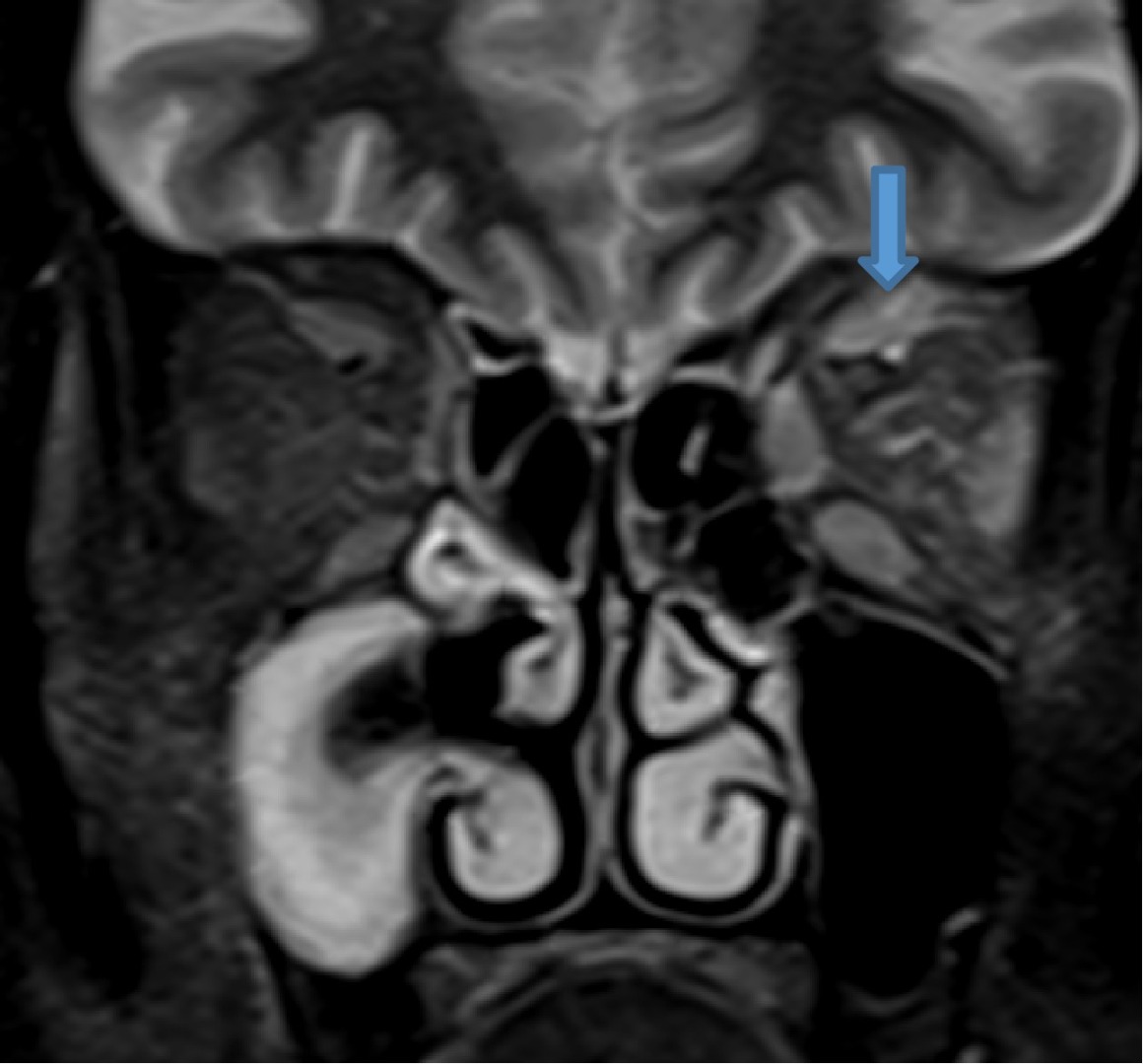
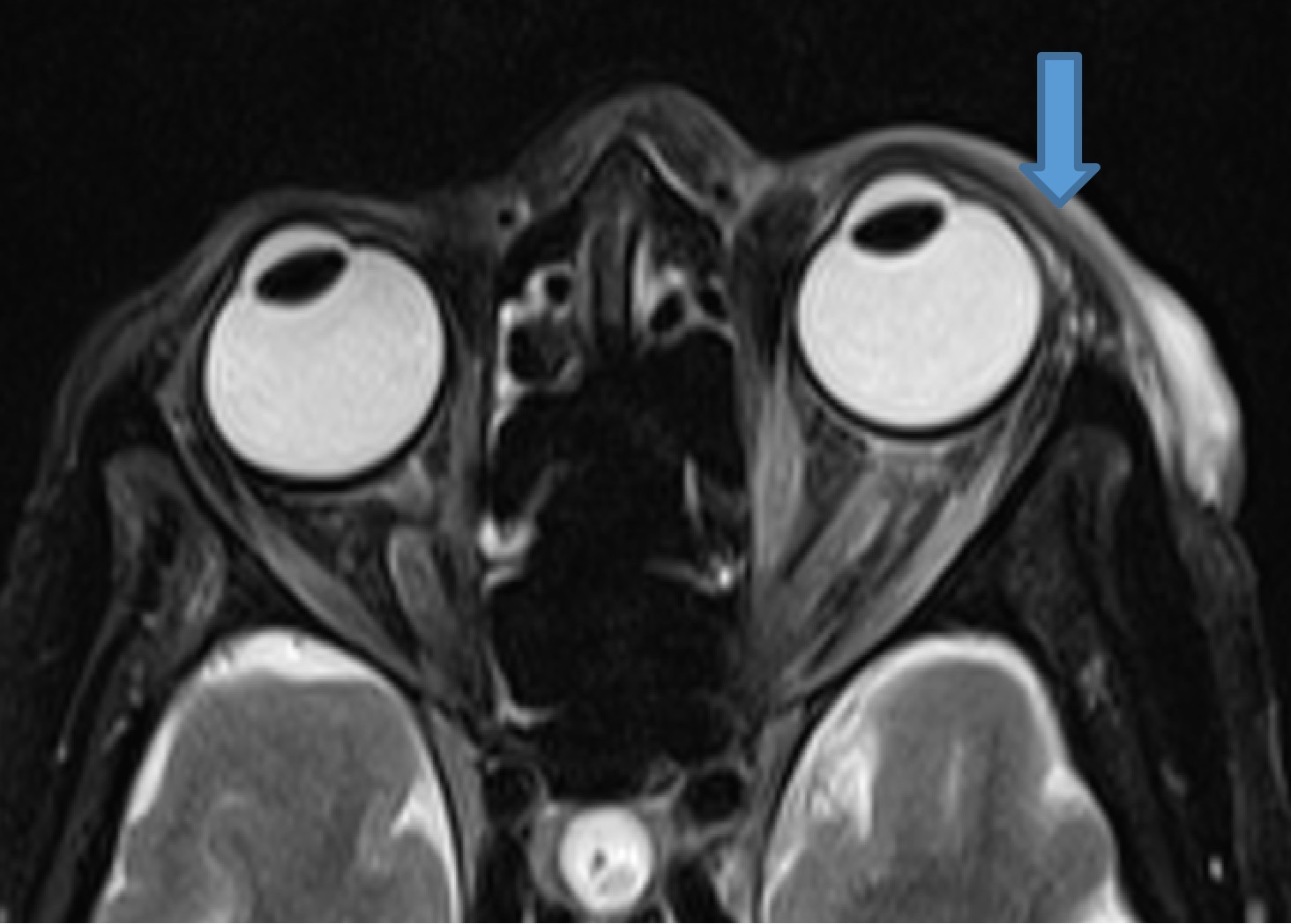
- Axial and coronal T2FS and post contrast axial T1FS
B.LEGENDS
- Bulky and enhancing extra-ocular muscles on left side
- Mild diffuse edema with thickening and post contrast enhancement in left preseptal space with mild fat stranding in the intraconal fat
- Mild left perioptic fat stranding and subtle post contrast enhancement of nerve sheath
- Mild congestive changes seen as increased enhancement of the left orbital apex

DIAGNOSIS
Left herpes zoster ophthalmicus with orbital myositis and optic perineuritis.
DISCUSSION
- Herpes zoster ophthalmicus (HZO) represents a vision-threatening reactivation of latent varicella-zoster virus within the ophthalmic branch of the trigeminal nerve.
- This condition accounts for a significant proportion of herpes zoster cases and carries a disproportionately high risk of ocular and neurologic morbidity.
- Clinical manifestations range from painful cutaneous eruptions across the ophthalmic dermatome to serious intraocular and orbital complications, including keratitis, uveitis, scleritis, retinitis, and optic neuropathy.
Pathophysiology of Ocular Involvement
- Once reactivated, VZV replicates and travels along sensory axons to the ophthalmic dermatome, producing the classic painful vesicular rash on the forehead, eyelid, and nose. Viral particles and immune-mediated inflammation extend into ocular tissues, where they can cause:
- Conjunctivitis and episcleritis (early involvement)
- Keratitis (epithelial, stromal, or neurotrophic) due to direct viral cytopathy and immune response
- Anterior uveitis from viral antigen-induced inflammation
- Retinitis, optic neuritis, and vasculitis in severe or disseminated cases
Key Radiological Findings
- MRI (Orbit/Brain): Typically shows enhancement of the optic nerve (optic neuritis), thickened or inflamed extraocular muscles (orbital myositis), and enhancement of cranial nerves III, IV, V, or VI
- Orbital Apex Syndrome: MRI may reveal inflammation, enhancement, or soft tissue density at the orbital apex, causing multiple cranial nerve dysfunctions
- Intracranial Involvement: MRI/MRA can detect VZV-induced vasculitis, stroke, or, rarely, encephalitis.
- Orbital Cellulitis: Imaging helps differentiate preseptal from postseptal orbital cellulitis, showing fat stranding and extraocular muscle enlargement.
Complications
- Orbital Myositis: Often appears as swelling and enhancement of one or more extraocular muscles.
- Ophthalmoplegia: Caused by cranial nerve palsy or direct muscle inflammation, visualized on neuroimaging.
- Optic Neuritis: Indicated by high signal intensity on T2-weighted MRI and contrast enhancement of the optic nerve.
- Stroke: Risk is 4.3 times higher within one year post-infection, often secondary to vasculitis.
Management
- Supportive care
- Antiviral agents
- Antibiotics
- Corticosteroids
- Topical aqueous suppressants
- Debridement
REFERENCES
https://www.ncbi.nlm.nih.gov/books/NBK557779/
By Kathryn Lewis, BS, Bea Palileo, MS, Charles Pophal, BS, Joseph Yasmeh, BS, and Ray Glendrange, MD Edited By: Ingrid U. Scott, MD, MPH, and Bennie H. Jeng, MD
Zhou Wenting, Sandy, and Srinivasan Sanjay. 2014. “Role of Magnetic Resonance Imaging in Herpes Zoster Ophthalmicus Ophthalmoplegia”. Ophthalmology Research: An International Journal 2 (4):189-95. https://doi.org/10.9734/OR/2014/8098.
Dr. Neha Sathyanarayana
Radiology Resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr. Anita Nagadi
Senior Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.