A 33 year old male with swelling on the back of the neck. On external examination no erythema over the swelling, non-tender.
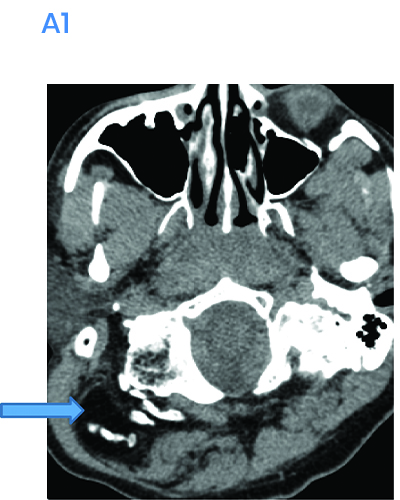
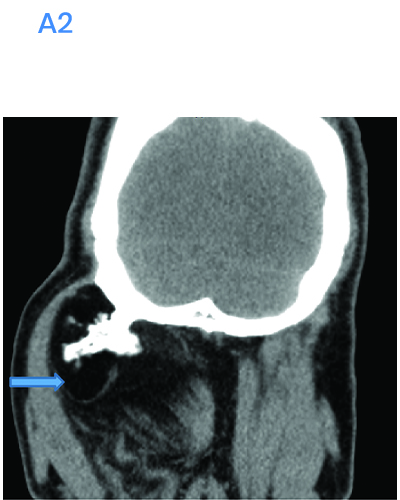
- A.FINDINGS – NCCT NECK, AXIAL, CORONAL AND SAGITTAL IMAGES
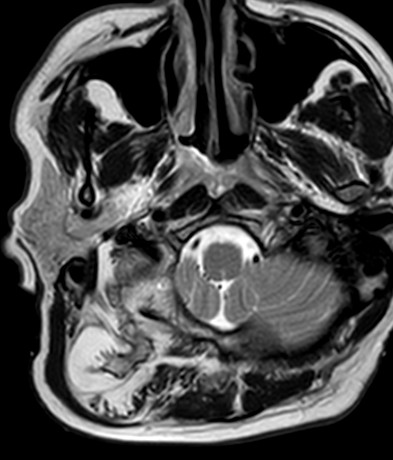
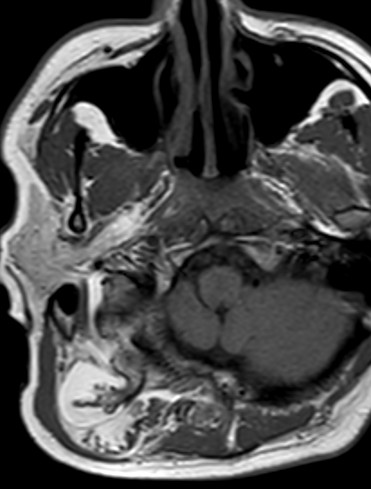
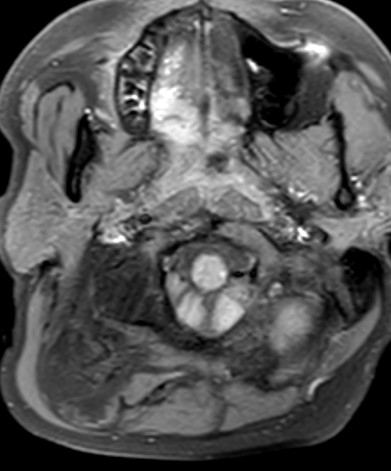
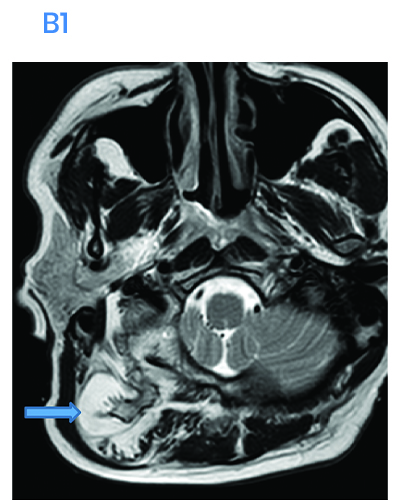
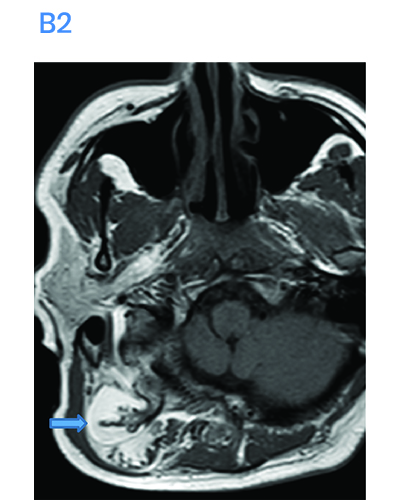
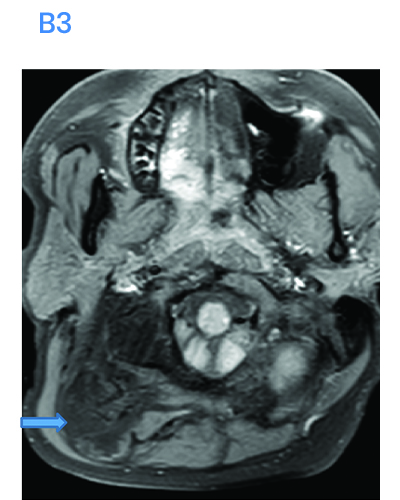
- B.FINDINGS – MRI AXIAL T2, T1 AND T1FS IMAGES OF NECK

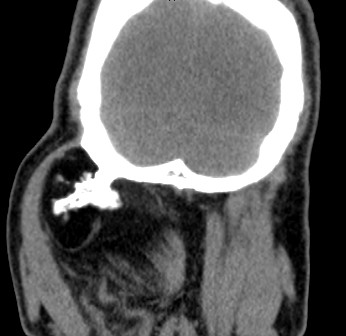
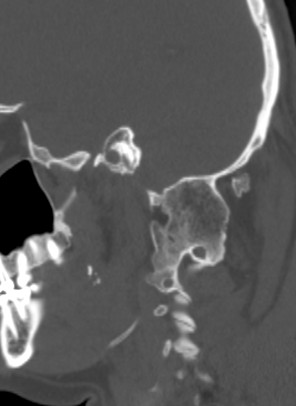
Legends A
- Large predominantly fatty attenuation swelling with central bony protruberance arising from the occiput and upper cervical vertebrae.
- Bony ankylosis seen between occipital condyle & C1 vertebrae bilaterally.
- Bony ankylosis also seen between the anterior arch of C1 and odontoid process as well as C1 and C2 vertebrae.
Legends B
- It is associated with atrophy of the paraspinal muscles on the right side & replaced by encapsulated fatty tissue.
- Chunks of ossific structure attached to the adjacent occipital bone is seen projecting into the hypertrophied fat in the right paraspinal space likely heterotopic ossification.

Diagnosis
- Right suboccpital osteolipoma with heterotrophic ossification.
Discussion
- Osteolipoma is an extremely rare variant, accounting for less than one percent of all lipomas found in the human body.
- According to the World Health Organisation (WHO) classification of soft tissue tumours, osteolipoma is a variant of lipoma.
- Terms such as ossifying lipoma, osseous lipoma, and lipoma with osseous metaplasia have been used interchangeably with osteolipoma. Consequently, many prior reports of “osteolipoma” included tumours which in actual fact are parosteal lipomas and intraosseous lipomas
- Parosteal lipomas are neoplasms of mature adipose tissues that are contiguous with underlying periosteal bones, commonly associated with reactive changes or hyperostosis in the underlying cortex whereas intraosseous lipomas are lipomas that arises within the medullary cavity and occasionally within the cortex of a bone.
- Osteolipoma however, can be classified according to the composition of its tissue content. It is called ossifying lipoma if the adipose component is the predominant tissue type, while the term osteolipoma is used if it contains more bony element.
Imaging:
- Computed Tomography (CT) with or without contrast is the most frequently used cross-sectional imaging to investigate osteolipoma. Radiologically, it is a well-defined, heterogenous mass with mixed density.
- Its overall appearance is dependent on the predominant make-up of the tumour.
- Tumours which are clinically soft and consist of mainly fatty tissue appear as hypodense mass (fat attenuation centrally) with peripheral hyperattenuation.
- Internal septations can occasionally be observed.
- Conversely, tumours which are clinically firm and hard would appear as a hyperdense mass with central calcified portion and focal areas of fat attenuation
Management
- As a benign, indolent and slow growing neoplasm, osteolipoma can potentially be managed conservatively.
- Complete surgical excision.
References:
Wong BLK, Hogan C. Osteolipoma of head and neck - a review. Braz J Otorhinolaryngol. 2022 Nov-Dec;88 Suppl 4(Suppl 4):S177-S187. doi: 10.1016/j.bjorl.2022.04.002. Epub 2022 May 20. PMID: 35659712; PMCID: PMC9756048.
https://www.jprasurg.com/article/S0007-1226(03)00096-1/fulltext
Dr. Neha Sathyanarayana
Radiology Resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr. Anita Nagadi
Senior Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.