

A 36 years old female, 7 days post-partum developed severe abdominal pain.
A 36 years old female, 7 days post-partum developed severe abdominal pain.
- O/E: Well healed wound.
FINDINGS:
- CT ABDOMEN AND PELVIS WITH CONTRAST AXIAL AND CORONAL IMAGES
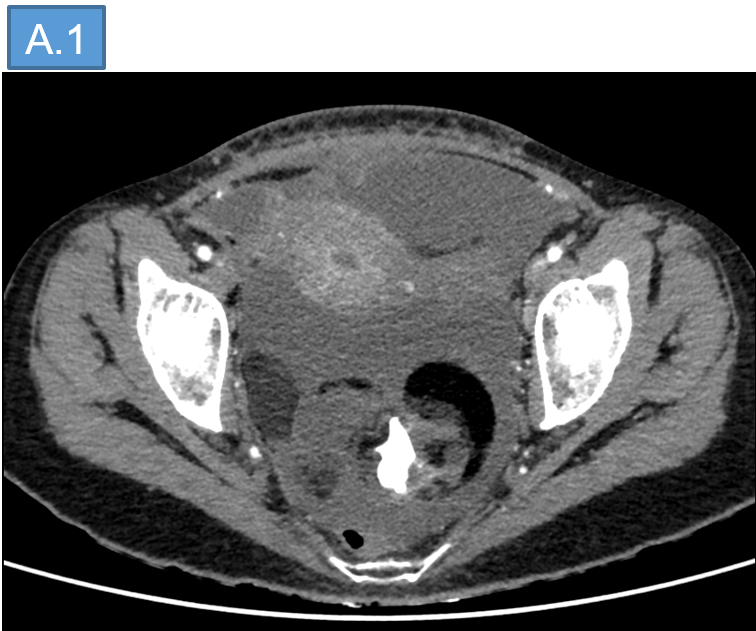
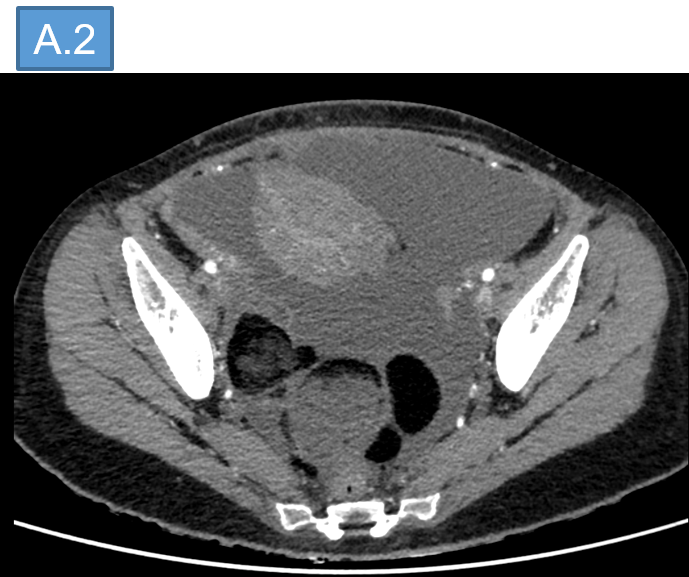

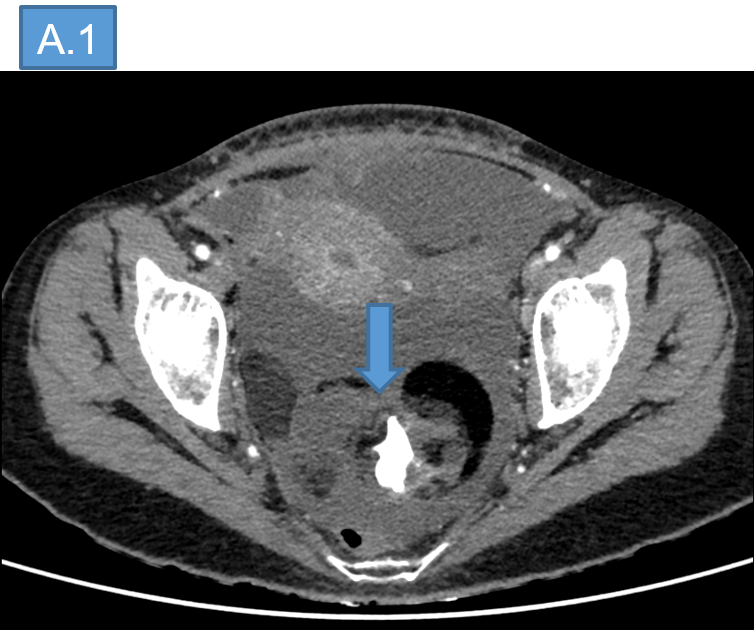
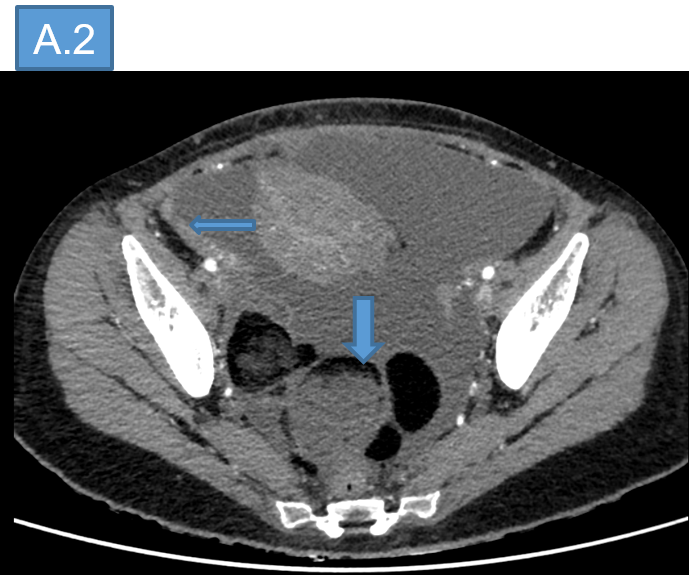
- Relatively well-defined large heterogeneous lesion in the pelvis. Fat component and calcifications are seen within the lesion. Left ovary is not separately visualized.
- Moderate ascites (with fatty fluid), diffuse omento-mesenteric fat stranding and thickening of the peritoneal layers.
- Few fat density foci are seen under the dome of right diaphragm.

DIAGNOSIS:
- Ruptured dermoid cyst with chemical peritonitis.
DISCUSSION:
- Ovarian teratomas are the most common type of germ cell tumors (GCT).
- Ovarian teratomas may be subdivided into mature teratomas, immature teratomas and monodermal teratomas.
- Mature teratoma, also known as dermoid cyst, is the most common subtype of ovarian teratomas constituting >95% of all teratomas and 69% of all germ cell tumors.
- Although mature teratomas may arise in any age group, this tumor has a predilection for women of reproductive age and is the most common adnexal mass in pregnant woman.
| MATURE TERATOMA | IMMATURE TERATOMA |
| Clinically benign | Clinically malignant |
| Well defined capsule | Frequently exhibit perforation of capsule |
| Average size 7cm | Typically larger average size ~ 14cm |
| HPE: contain well differentiated endodermal, ectodermal, and mesodermal tissues | HPE: differ from mature teratomas by demonstrating presence of embryonic elements, most commonly primitive neuroepithelium |
| Unilocular cysts that may have septa and a prominent raised protuberance called the Rokitansky nodule or dermoid plug. | Completely solid or mostly solid with some cystic components. The cystic components are usually composed of sebaceous, mucinous, or serous fluids |
- In monodermal teratomas, a single element constitutes most of the tumor giving rise to three different subtypes (neuroectodermal, struma ovarii, and carcinoid).
COMPLICATIONS OF TERATOMAS:
- Rupture: Spontaneous rupture in ovarian teratomas occurs in only 3.8% of cases due to a thick capsule. Acute perforation can be seen on imaging as a discontinuation of the tumor’s wall or as distortion of the tumor that may lead to a flattened appearance. CT may show hemoperitoneum, along with free floating fat globules.
- Torsion
- Malignant transformation
- Growing Teratoma syndrome
- Anti - NMDA Encephalitis
Management:
- Emergency laparotomy – removal of the cyst and fat droplets.
REFERENCES:
- Ruptured intracranial dermoid cysts: a pictorial review 2018 Oct 19;83:e465–e470. doi: 10?5114/pjr?2018?80206
- Remote rupture of ovarian dermoid cyst: A curious case report https://doi?org/10?1016/j?radcr?2024?09?142
Dr MADHUKUMAR S
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr NEHA SATHYANARAYANA
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
