
A 35-year-old presenting with complaints of intermittent claudication pain in left lower leg.
History
A 35-year-old presented with complaints of intermittent claudication pain in the left lower leg. History of similar complaints 10 years ago in the right lower leg and was found to have right popliteal artery thrombosis and graft replacement surgery was done.
Investigation – CT- Lower limb peripheral angiography was performed.
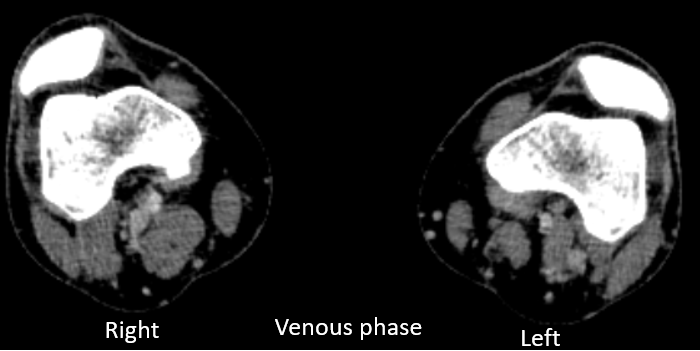

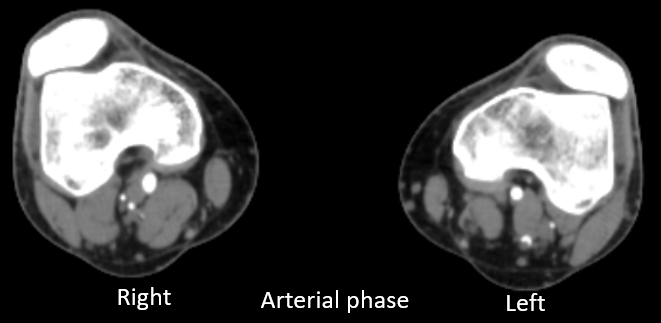
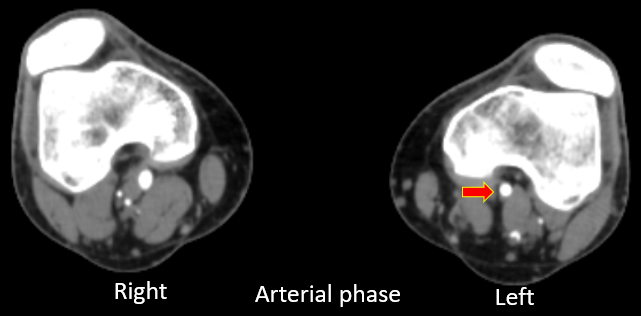
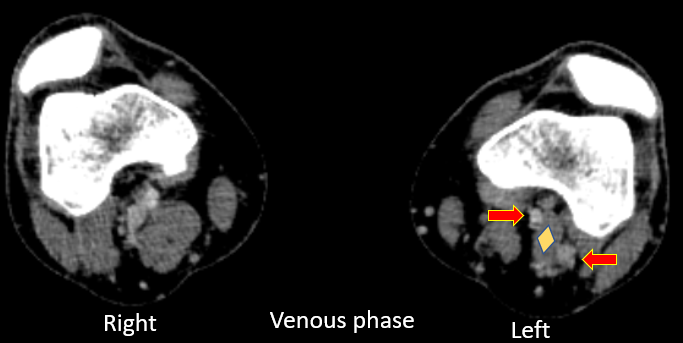
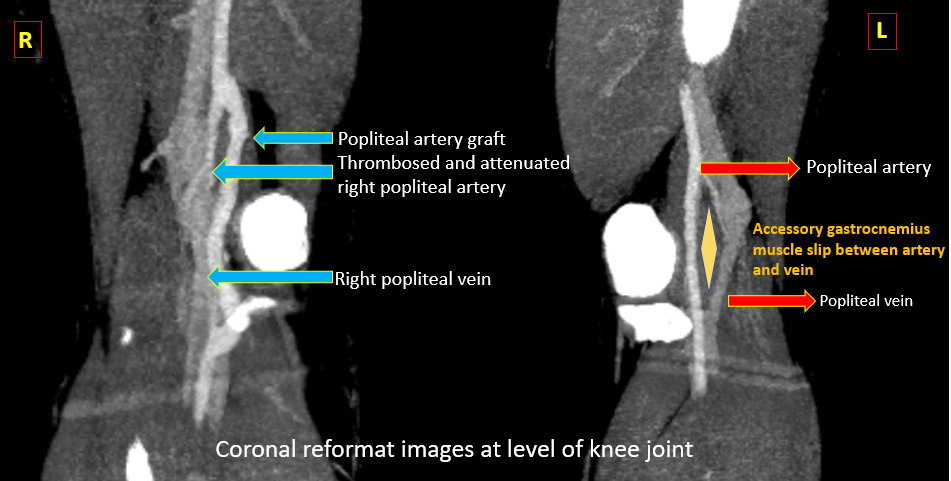
- CT peripheral lower limb angiography AXIAL images (image 1 and 2) at the level of popliteal fossa demonstrates diastasis between the left popliteal artery and vein with an accessory muscle slip coursing between the artery and vein at the level of popliteal fossa in left leg.
- CT coronal image (image 3) demonstrates the origin of this accessory slip from medial head of left gastrocnemius and inserts onto femoral condyle.
- No abnormal medial deviation of left popliteal artery or vessel wall irregularity or intraluminal filling defect in left popliteal artery.
- Chronic occlusion of right popliteal artery secondary to right popliteal artery entrapment syndrome and underwent surgical treatment, with normal contrast opacification within the graft.
DIAGNOSIS AND DISCUSSION:
- Abnormal course of left popliteal artery between two slips of medial head gastrocnemius muscle suggestive Popliteal artery entrapment syndrome (PAES)of left lower leg.
- CTA or MRA can be done to identify abnormal tendinous or muscular structures, an insertion anomaly and/or arterial deviation. Aberrant muscular and fibrous attachments can be different in almost every case and it best evaluated on axial images.
- Doppler ultrasonography is useful is dynamic assessment of popliteal artery by performing plantar flexion and useful in assessing the changes in flow dynamics in the artery.
- In our case, an accessory muscular slip from medial head of gastrocnemius was seen between the popliteal artery and vein suggestive TYPE III PAES.
- Arterial compression can result in chronic vascular microtrauma, local premature arteriosclerosis, and thrombus formation. This can result in distal ischemia. Stenosis and turbulent flow may lead to post-stenotic ectasia or aneurysm formation.
Discussion:
- PAES – symptomatic compression or occlusion of popliteal artery due to a developmentally abnormal positioning of the popliteal artery in relation to its surrounding structures such as with the medial head of gastrocnemius or less commonly with popliteus or fibrous bands.
Delaney et al classified PAES into four types:
Type 1 – The popliteal artery is abnormally running medial to the medial head of the gastrocnemius, which has a normal insertion.
Type 2 – Entrapment results from an aberrant insertion of the medial head of the gastrocnemius muscle.
Type 3 – Entrapment results from an accessory slip from the medial head of the gastrocnemius muscle.
Type 4 – The popliteal artery is compressed when passing under the popliteal muscle or under a fibrous web.
- Popliteal artery entrapment syndrome is an uncommon entity typically affecting young athletic males who present with symptoms of calf claudication. It is caused by an anomalous relationship of muscle and artery in the popliteal fossa resulting in extrinsic arterial compression. Repetitive insult to the popliteal artery can cause arterial damage and lead to aneurysm, thromboembolism, and arterial thrombosis.
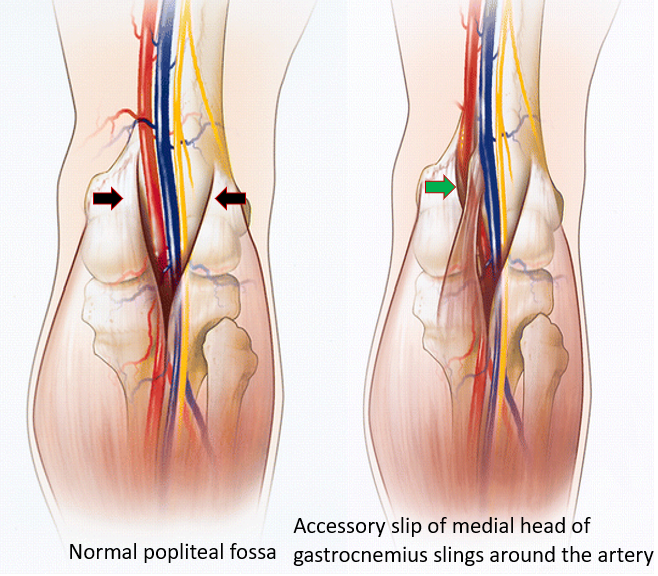
- The anomalous anatomic relationship responsible for compression of the popliteal artery is caused by abnormal embryologic development of the popliteal fossa. The muscle or the artery can be responsible for the abnormal anatomy, and numerous variations can result. It is important to recognize the normal appearance of the popliteal fossa anatomy
- Management – In case of acute limb-threatening thrombosis – urgent bypass surgery is necessary which the patient had underwent on the right leg. In case of intermittent occlusion, surgical release of the popliteal artery alone by resection/reposition of abnormal course of muscle/tendon/fibrous band or popliteal artery reconstruction with saphenous vein bypass can be considered.
References:
- Thanila A, Johnson CM, Hallett Jr JW, Breen JF. Popliteal artery entrapment syndrome: role of imaging in the diagnosis. AJR Am J Roentgenol. 2003;181:1259-65.
- Jarraya, M., Simmons, S., Farber, A., et al. Uncommon Diseases of The Popliteal Artery: A Pictorial Review. Insights Imaging 7, 679–688 (2016).
- Delaney TA, Gonzalez LL (1971) Occlusion of a popliteal artery due to muscular entrapment. Surgery 69:97–101
DMRD, DNB, EDiR
Consultant Radiologist
Manipal Hospitals Radiology Group
Dr. Diwakar C
Radiology resident
Manipal Hospitals Radiology Group
