A 12-year-old male patient complains of neck swelling with pain and dysphagia for 1 month
- 12 yr old male patient complains of neck swelling with pain and dysphagia for 1 month.
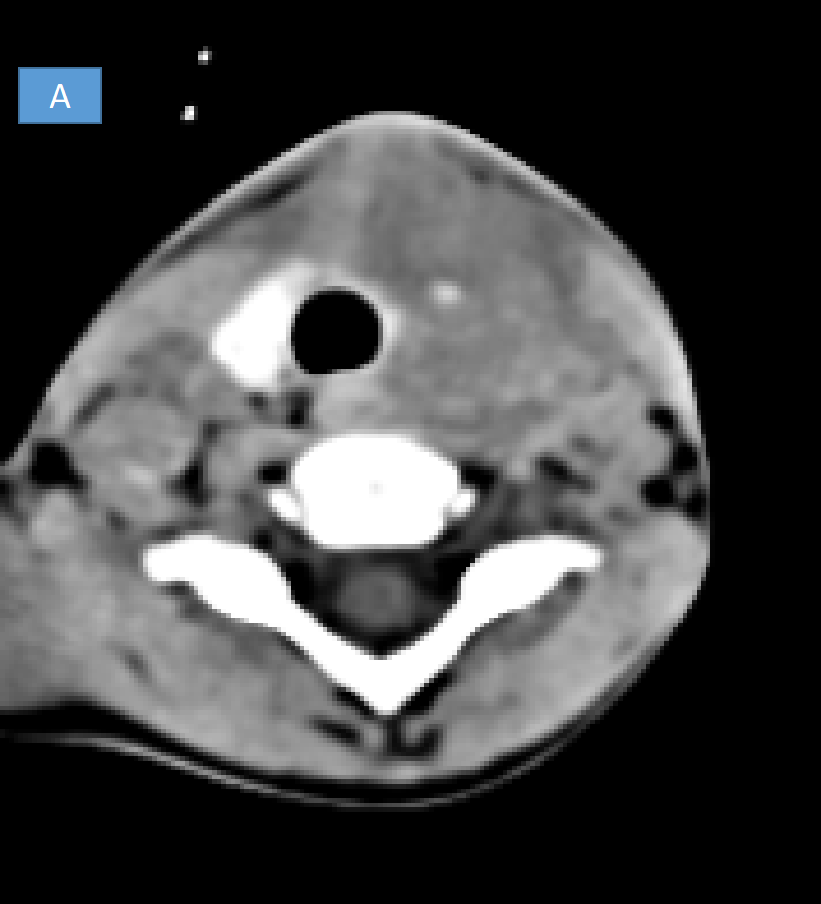

- A. Heterogeneous soft tissue density lesion in the left lateral aspect of infra-hyoid neck deep to the sternocleidomastoid involving the left thyroid gland.
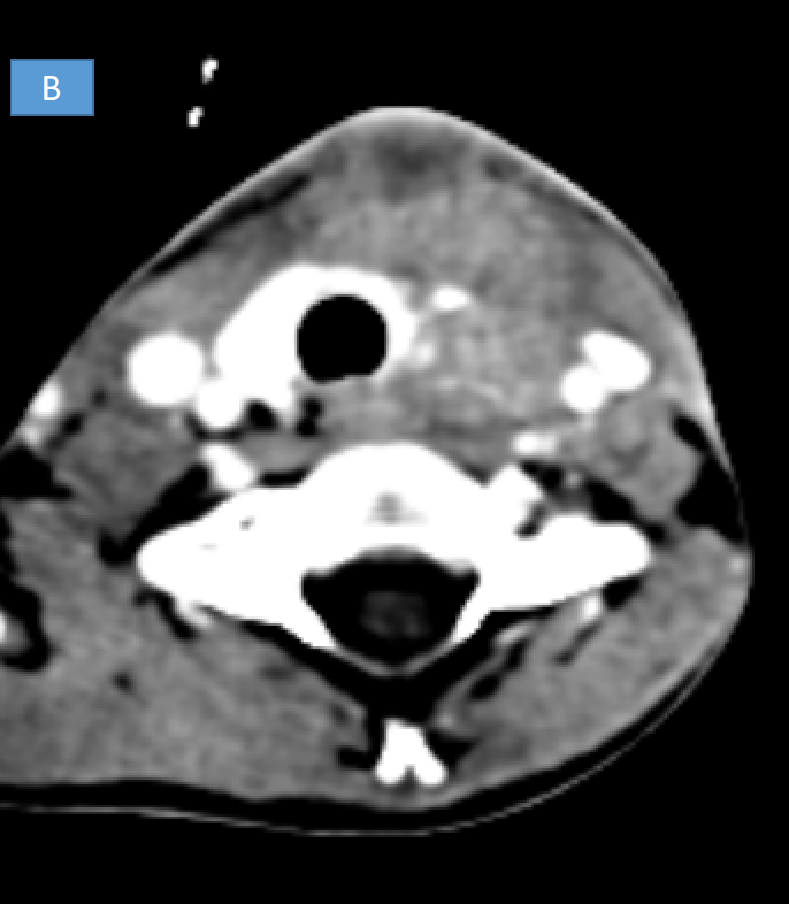
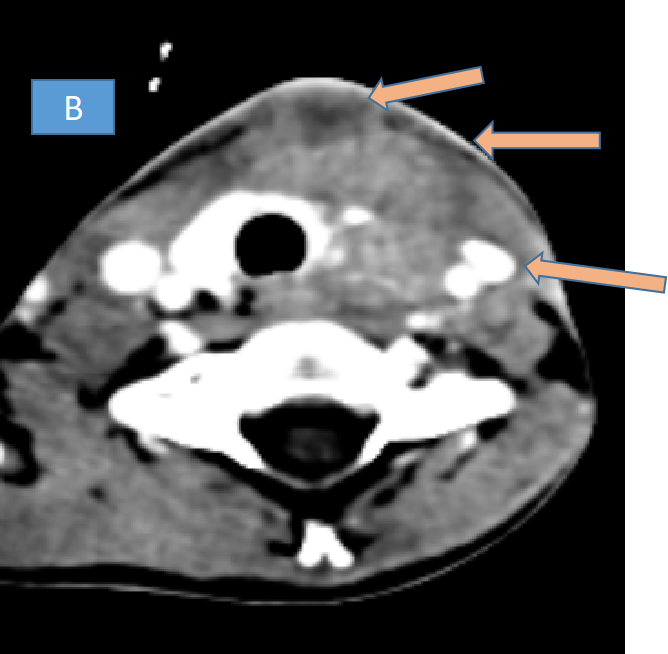
- B. Heterogeneous enhancement of the lesion seen with hypodense cystic areas and significant surrounding fat stranding and thickening of the platysma muscle. Fat stranding and edema is also noted in the left carotid space.
- C. Lesion encases the left lobe of thyroid and reaches till the skin.
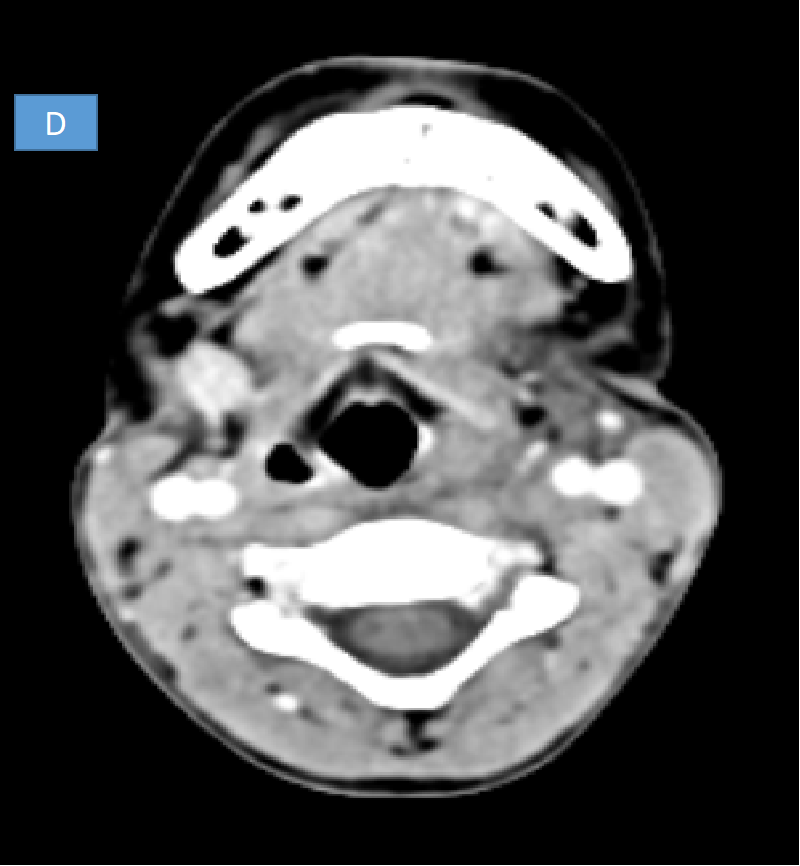
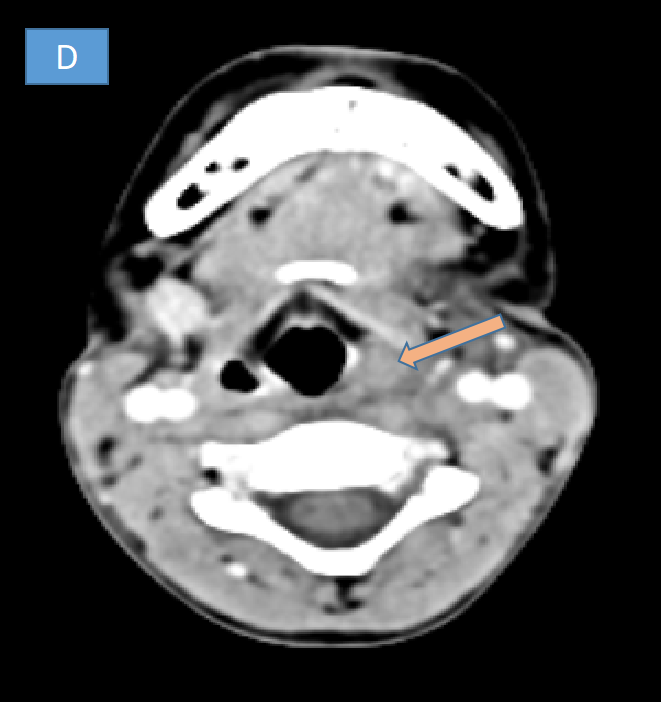
- D. Superiorly there is soft tissue thickening and edema in the trachea-esophageal groove and left side pyriform fossa which is seen effaced.


DIAGNOSIS
- THIRD/FOURTH BRANCHIAL CLEFT CYST
DISCUSSION
- Branchial cleft anomalies arise from incomplete obliteration of any branchial tract, resulting in either a cyst (75%) or a sinus or fistulous tract (25%).
- First branchial cleft anomalies are relatively less common and typically closely related to the parotid gland. These commonly present as fistula and sinus, whereas cysts are least common.
- Most common type is 2nd branchial cleft cyst and usually present as a cystic mass.
- Third and fourth branchial cleft anomalies are exceedingly rare and typically present with a long history of neck infections. Both are related to the pyriform sinus.
- Cysts at the level of the thyroid gland can be remnants of the third or fourth branchial cleft.
THIRD BRANCHIAL CLEFT CYST
- Most commonly on the left side.
- Posterior to the common or internal carotid artery, between the hypoglossal nerve below and the glossopharyngeal nerve above .
- Posterior cervical space, posterior to the sternocleidomastoid muscle.
- If sinus formation- drain into the pyriform sinus.
FOURTH BRANCHIAL CLEFT CYST
- Parallel the course of the recurrent laryngeal nerve.
- Most commonly on the left side (80%). Most common presentation is abscess within or anterior to the left thyroid lobe.
- If sinus formation- drain into the apex of pyriform sinus., but passes inferiorly rather than superiorly to reach anterior left upper thyroid lobe.
- The proximity of the third and fourth branchial arches makes distinguishing third from fourth branchial cleft abnormalities radiologically difficult.
- For an accurate diagnosis, the relationship of the sinus tract to the superior laryngeal nerve must be determined surgically.
FIRST BRANCHIAL CLEFT CYST
- There may be a sinus with drainage to the external ear or skin.
- Adjacent to the parotid gland or external auditory canal.
SECOND BRANCHIAL CLEFT CYST
- Type 1: Anterior to the sternocleidomastoid deep to the platysma.
- Type 2: Most common variant, deep to the sternocleidomastoid and lateral to the carotid space.
- Type 3: Extend medially between the bifurcation of internal and external carotid arteries up to the lateral pharyngeal wall.
- Type 4: Pharyngeal mucosal space medial to the carotid sheath.
DIFFERENTIAL DIAGNOSIS FOR CYSTIC NECK MASSES IN CHILDREN

THYROGLOSSAL DUCT CYST
- Most common midline congenital neck mass (70%).
- Infrahyoid (most common)/level of hyoid bone / suprahyoid location.
- Deep to or embedded in the infrahyoid strap muscles.
- Presence of solid soft tissue elements, often nodular- highly suspicious of malignancy.
- Calcification within the cyst - specific finding of development of carcinoma.
LYMPHANGIOMA
- Cystic hygroma -most common form.
- Posterior triangle or the sub-mandibular space.
- Infiltrative in nature and do not respect facial planes.
- Posterior neck - one or more larger cysts.
- Anterior neck - innumerable small cysts,
- Mediastinum and axilla are common sites of their extension.
- Fluid-fluid levels may be present when the lesions are complicated by hemorrhage.
DERMOID CYSTS
- Manifest during the second and third decades of life.
- Sub-mandibular or sublingual space.
- Fat, mixed-density fluid and calcification .
- Coalescence of fat into small nodules within the cystic lesion- “sac-of-marbles” appearance.
EPIDERMOID CYSTS
- Most lesions evident during infancy.
- Floor of the mouth lesions- typically present as thin-walled, unilocular masses located in the sub-mandibular or sublingual space. The rim of the cyst may show contrast enhancement.
RANULAS
- Retention cyst from sublingual salivary gland.
- Extend through or over the mylohyoid muscle - "plunging ranula“ and can present as a submental or submandibular mass.
VENOUS MALFORMATIONS
- Low-flow vascular malformations.
- Characteristic imaging finding is presence of phleboliths.
- If lymphatic elements present- lymphaticovenous malformation- Fluid- fluid levels may be seen.
REFERENCES
- Adams A, Mankad K, Offiah C, Childs L. Branchial cleft anomalies: a pictorial review of embryological development and spectrum of imaging findings. Insights into imaging. 2016 Feb;7(1):69-76.
- Valentino M, Quiligotti C, Carone L. Branchial cleft cyst. Journal of Ultrasound. 2013 Mar;16:17-20.
- Gökçe E, Beyhan M. CT and MRI findings of branchial cleft cysts. Eastern Journal of Medicine. 2021;26(1):47-52.
- Kawaguchi M, Kato H, Aoki M, Kuze B, Hara A, Matsuo M. CT and MR imaging findings of infection-free and benign second branchial cleft cysts. La radiologia medica. 2019 Mar 13;124:199-205.
- Liberman M, Kay S, Emil S, Flageole H, Nguyen LT, Tewfik TL, Oudjhane K, Laberge JM. Ten years of experience with third and fourth branchial remnants. Journal of pediatric surgery. 2002 May 1;37(5):685-90.
- Guldfred LA, Philipsen BB, Siim C. Branchial cleft anomalies: accuracy of pre-operative diagnosis, clinical presentation and management. The Journal of Laryngology & Otology. 2012 Jun;126(6):598-604.
Dr. ANITA NAGADI
SENIOR CONSULTANT RADIOLOGIST
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU
Dr. JOMON SUNNY
FELLOW IN CROSS SECTIONAL IMAGING
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU