
63y Male, Had undergone fundoplication for severe Gastroesophegeal reflux disease 20 days ago
- 63y Male, Who Had undergone fundoplication for severe Gastroesophageal reflux disease 20 days ago.
- Now presenting with chest pain and breathing difficulties.
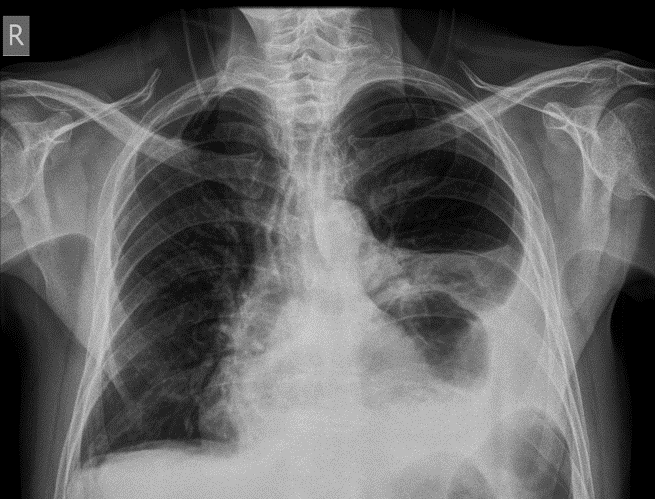



1. X-ray chest PA view showing large retro cardiac lucency with air-fluid level( green arrow) and opacity in left lower lung zone with blunted costophrenic angle (Orange arrow).
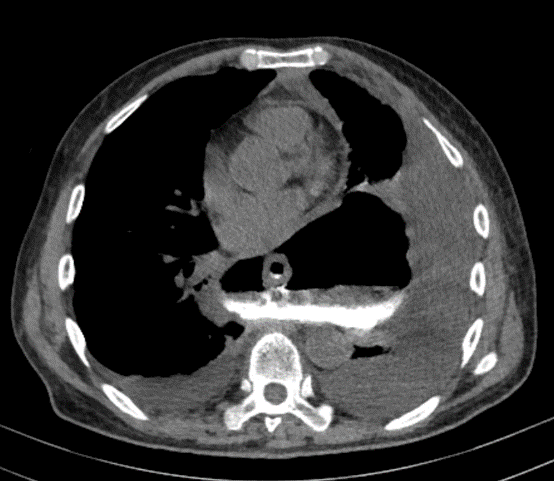
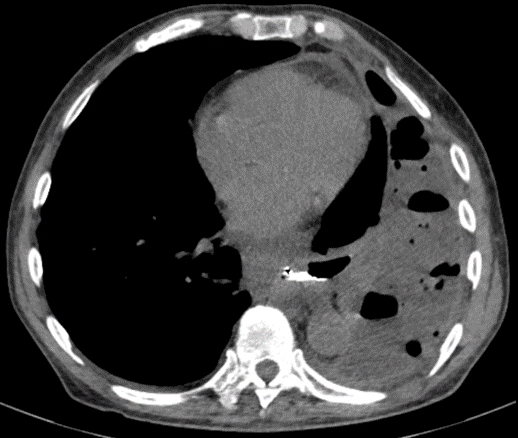
2. Plain CT chest in the mediastinal window with positive oral contrast in axial sections shows peri-esophageal fluid collection with evidence of air-fluid level around the lower end of the esophagus in the posterior mediastinum.
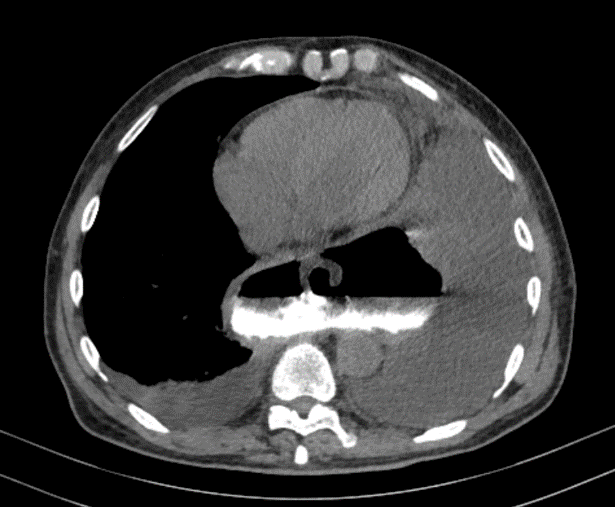
3. Changes of Collapse-consolidation changes in basal segments of the left lower lobe with bilateral pleural effusion (orange arrow).
4. Plain CT chest in the mediastinal window with positive oral contrast in the sagittal oblique section shows seepage of positive oral contrast into the collection across a defect (red arrow) in left postero-lateral of the esophagus.
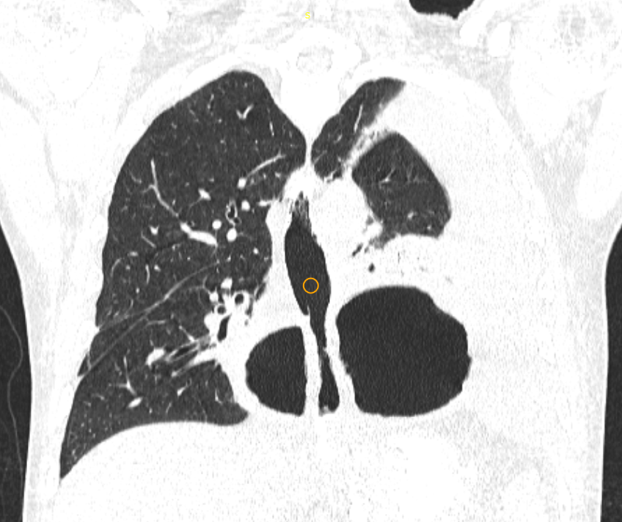
5,6. Plain CT chest in lung window with positive oral contrast in axial and coronal sections shows peri-esophageal fluid collection (blue arrow) with evidence of air fluid level around the lower end of the esophagus in the posterior mediastinum.
7,8. One month follow-up plain CT chest in the mediastinal window with positive oral contrast in axial sections shows a significant decrease in peri esophageal fluid collections and right-sided pleural effusion.
DISCUSSION:
Esophageal perforation is a rare but serious medical emergency with a very high mortality rate, especially if the diagnosis is delayed.
Epidemiology
Old age, slight male predominance.
Clinical presentation
Neck, chest or epigastric pain, dysphagia or dyspnea.
Subcutaneous emphysema may also be present.
Pathology
The lack of a serosal layer may make the esophagus more susceptible to injury than other parts of the gastrointestinal tract.
Etiology
- Iatrogenic: post-instrumentation or post-thoracic surgery (most common)
- complication of acute radiation-induced esophagitis
- Trauma/foreign body ingestion
- Corrosive material ingestion
- Oesophageal cancer
- spontaneous rupture post-vomiting (Boerhaave syndrome)
Radiographic features
Plain radiograph
- Pneumomediastinum, abnormal cardiomediastinal contour, pneumothorax and pleural effusion: although non-specific, for esophageal perforation.
- widening of the mediastinal shadow: non-specific on its own
Fluoroscopy
- most sensitive within the first 24 hours.
- patient examined semi-supine (~20 degrees) on the fluoroscopy table
- A low-osmolar water-soluble agent should be used initially as barium can cause mediastinitis
- esophageal perforation may be represented as mucosal irregularity or extra luminal oral contrast leak
CT
- Extra luminal gas locules in the mediastinum or abdominal cavity, adjacent to the esophagus: highly suggestive.
- Pleural or mediastinal fluid
- Pneumomediastinum or pneumothorax
- Water-soluble oral contrast can be administered 20 minutes before scanning to demonstrate extraluminal contrast leak.
- Intravenous contrast is usually administered to delineate the esophageal wall (25-60-second delay).
Complications
- Acute mediastinitis.
- Oesophagopleural fistula.
- Pneumonia.
- Empyema.
- Sepsis.
CT Esophagography:
- CT study is designed to primarily evaluate the esophagus, particularly in the situation of esophageal trauma and potential perforation. It has been developed partly as an alternative to fluoroscopic barium swallow evaluation in this situation.
- CT esophagography is relatively sensitive and highly specific for the evaluation of acute esophageal injury, including penetrating trauma, post-anastomotic leak, and esophageal rupture.
- CT esophagography has been shown to be at least equal to fluoroscopic esophagography for diagnosis of esophageal injury, with the key advantage of 24-hour and 7-day-a-week availability in most hospitals.
- The hallmark finding of esophageal injury or leak is extra luminal contrast material. In the absence of oral contrast material administration, peri esophageal air collections are the next most useful finding for depicting pathologic conditions
- CT is superior to fluoroscopic esophagography for the depiction of peri-esophageal collections.
- In addition, CT may help assess the presence of peri esophageal inflammation and may demonstrate intramural esophageal air, suggesting non transmural tears (Mallory-Weiss tears), which are likely to be fluoroscopically occult.
Reference :
- Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Lippincott Williams & Wilkins. (2007) ISBN:0781761352.
- Emergency Radiology. Springer. (2007) ISBN:3540689087.
- Chung DYF, Mondal D, Holmes EJ et al. Emergency cross-sectional radiology. Cambridge University Press. ISBN:0521279534.
- Gore RM, Levine MS. High Yield Imaging: Gastrointestinal: Expert Consult – Online and Print, 1e (HIGH YIELD in Radiology). Saunders. ISBN:1416055444.
- Søreide JA, Viste A. Esophageal perforation: diagnostic work-up and clinical decision-making in the first 24 hours. Scand J Trauma Resusc Emerg Med. 2011;19 (1): 66. doi:10.1186/1757-7241-19-66- Pubmed citation
- Hasimoto CN, Cataneo C, Eldib R et-al. Efficacy of surgical versus conservative treatment in esophageal perforation: a systematic review of case series studies. Acta Cir Bras. 2013;28 (4): 266-71. doi:10.1590/S0102-86502013000400006 – Pubmed citation
- Giménez A, Franquet T, Erasmus JJ et-al. Thoracic complications of esophageal disorders. Radiographics. 2002;22 Spec No (suppl 1): S247-58. Radiographics (full text)– doi:10.1148/radiographics.22.suppl_1.g02oc18s247 – Pubmed citation
Dr. Deepthi H V
Consultant radiologist.
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.
Dr. Srinivas P
Fellow in Radiology
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.
