
57 year old female presented with dyspnoea on exertion since 1 month and Wheezing
57 year old female presented with dyspnoea on exertion since 1 month and Wheezing
FINDINGS:
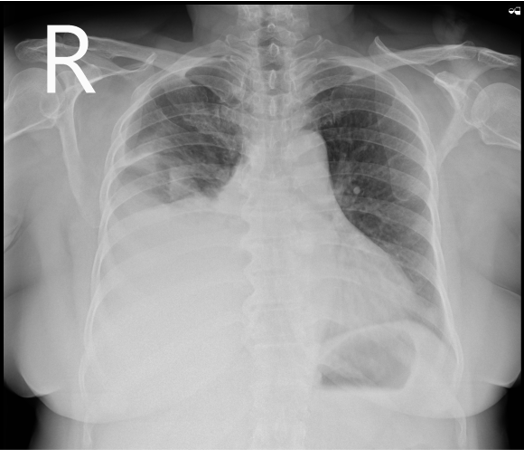
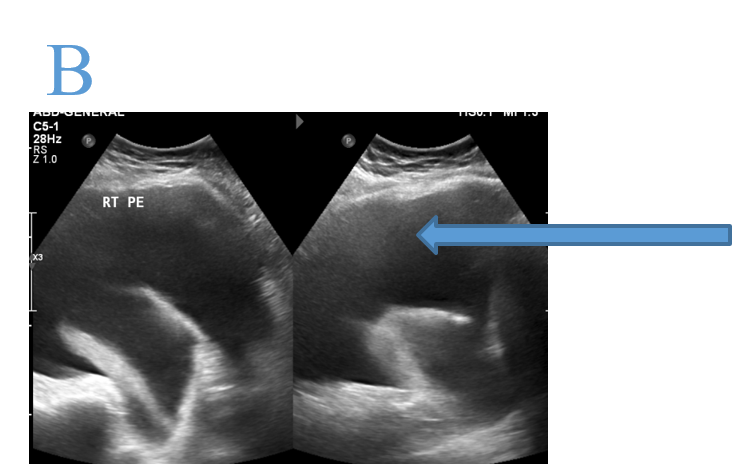
- X RAY CHEST PA
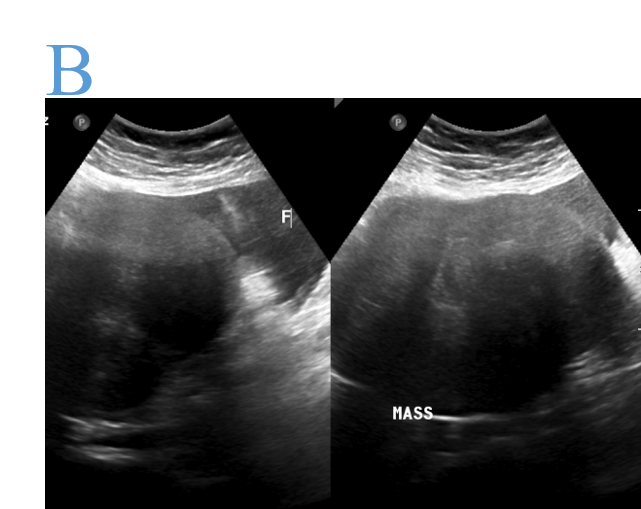
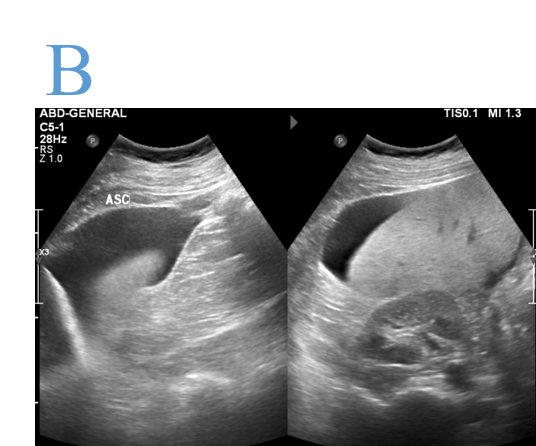
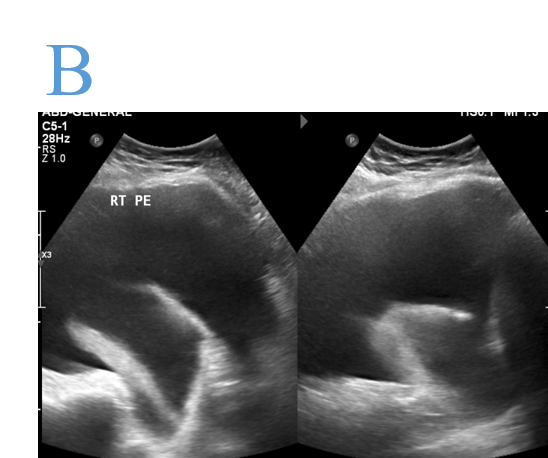
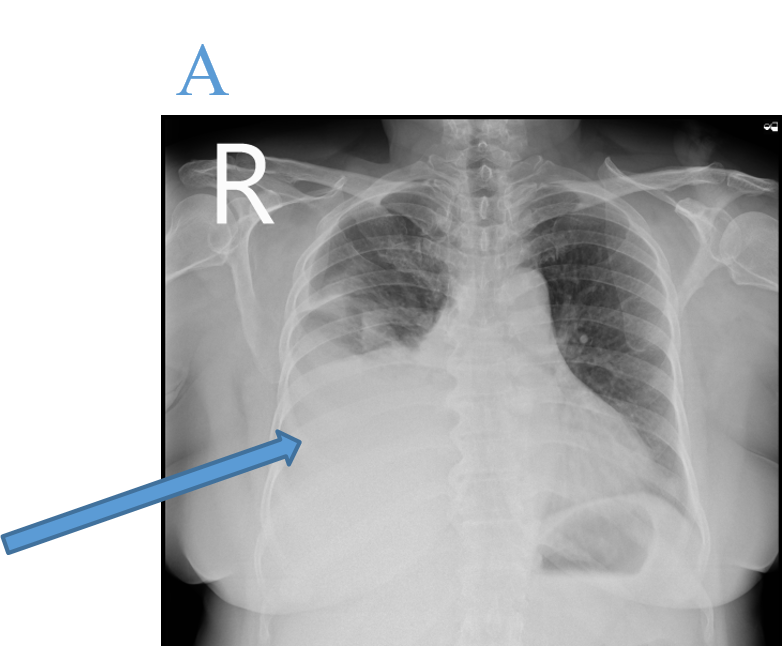
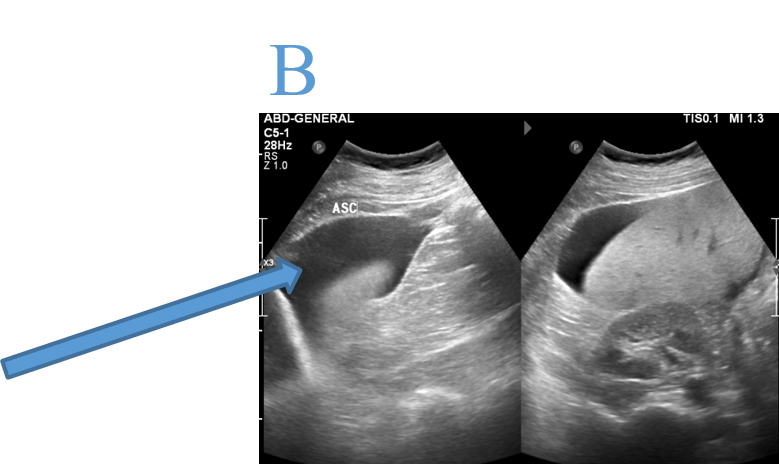
- USG ABDOMEN AND PELVIS
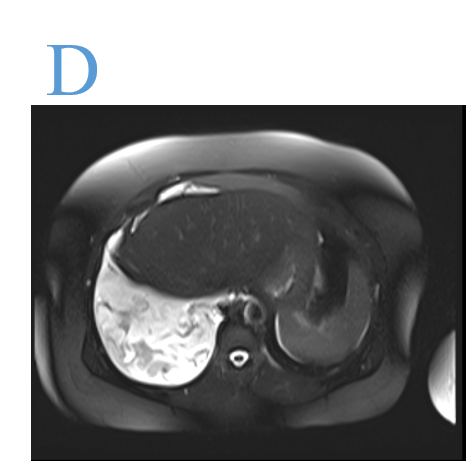
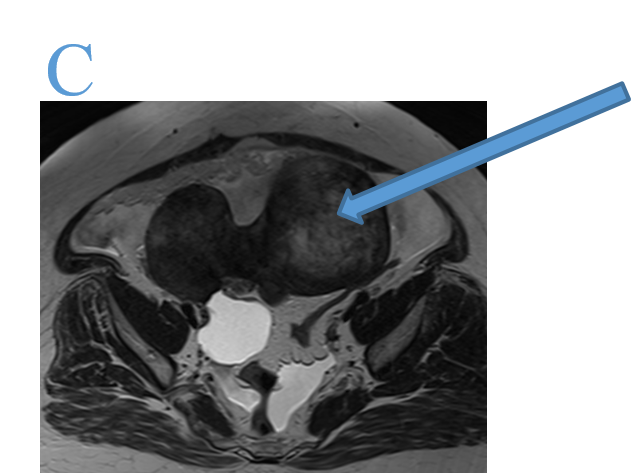
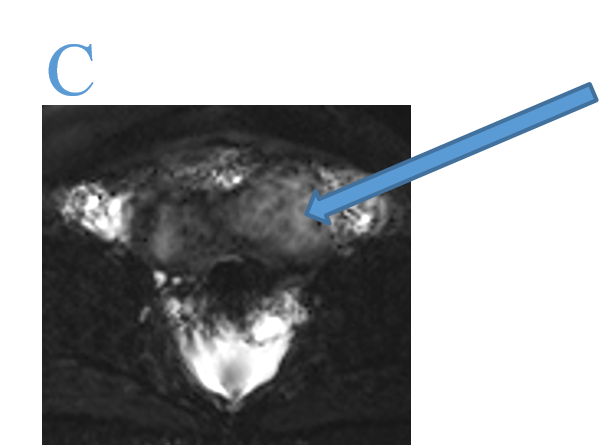
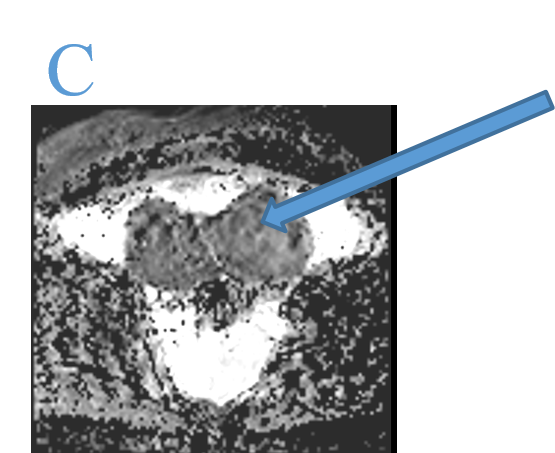
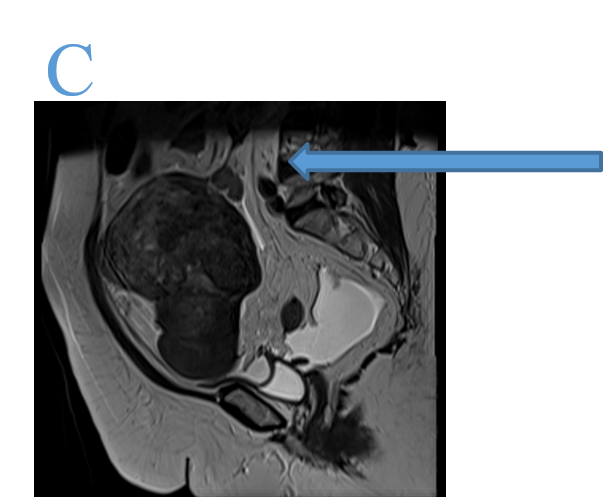
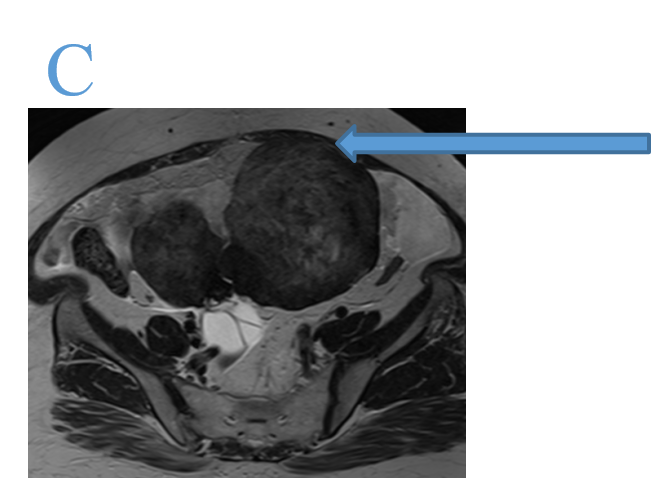
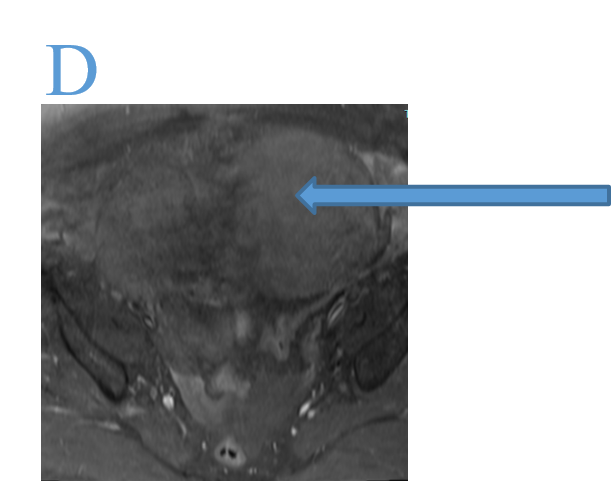
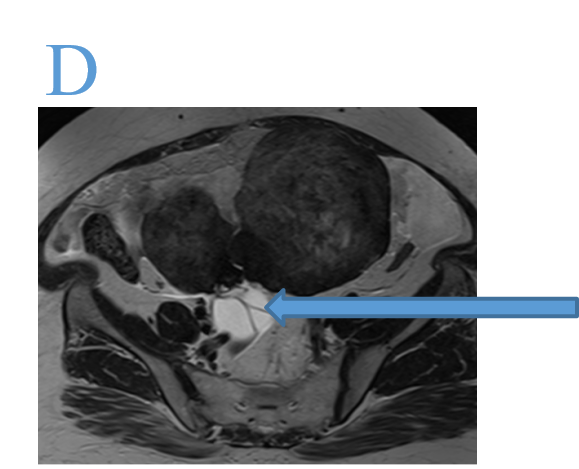
- MR ABDOMEN AND PELVIS WITH CONTRAST


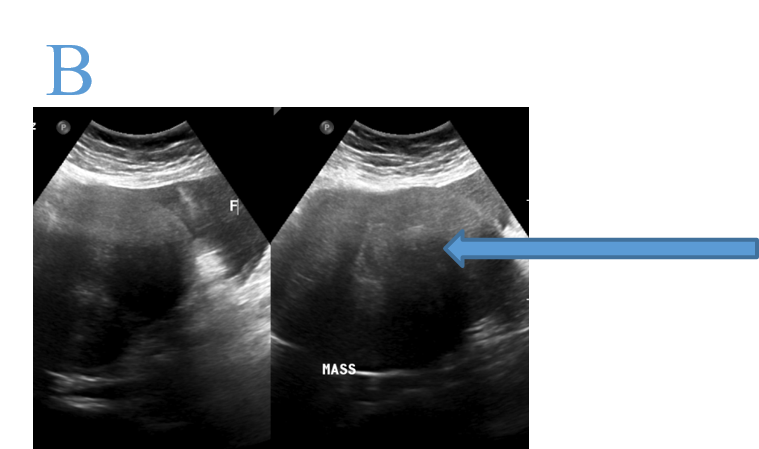
- Right sided moderate pleural effusion.
- Large lobulated solid hypoechoic lesion in the lower abdomen.
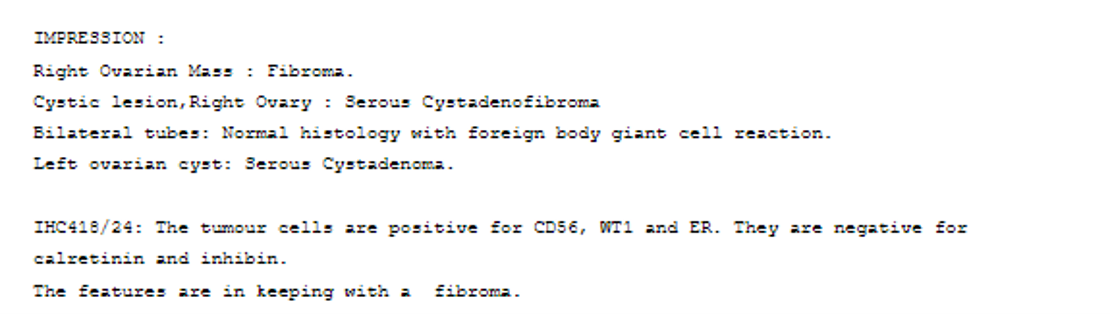
- Right sided moderate to large pleural effusion.
- Moderate ascites.
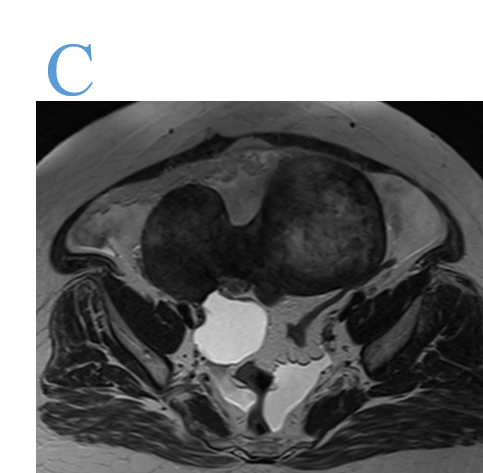
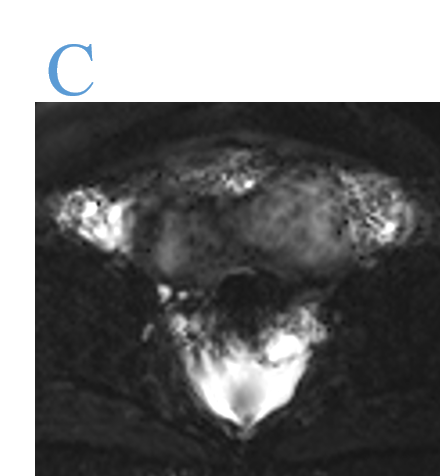
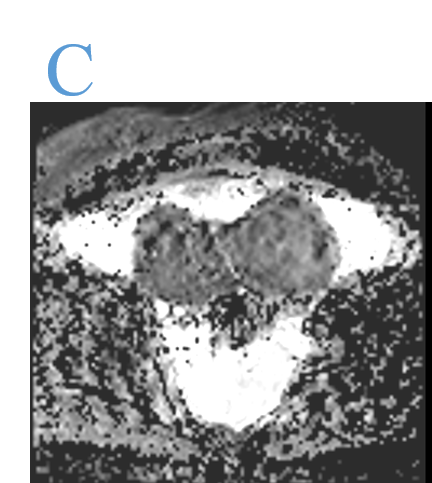
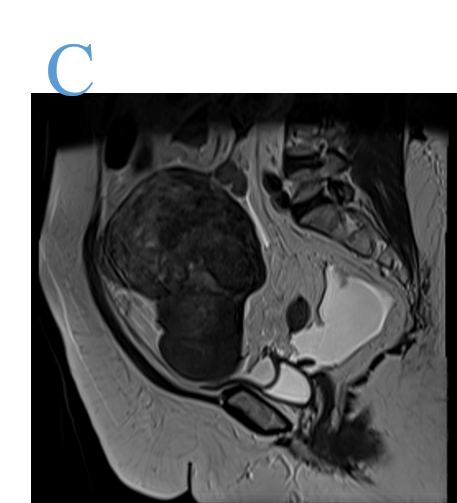
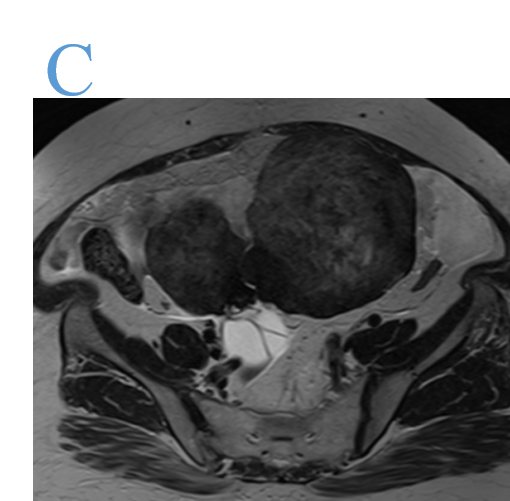
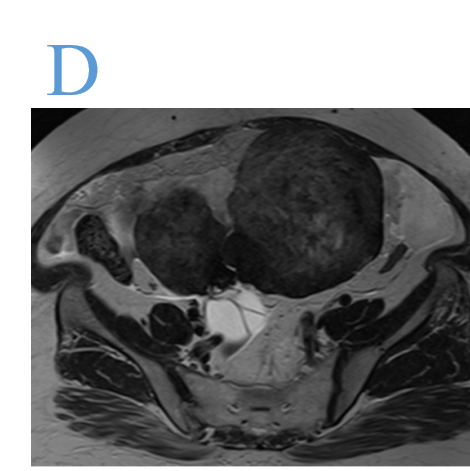
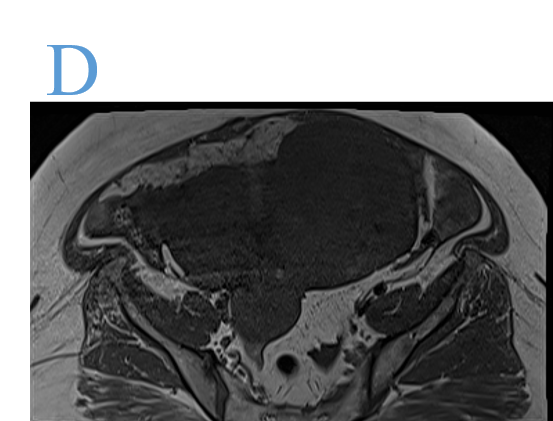
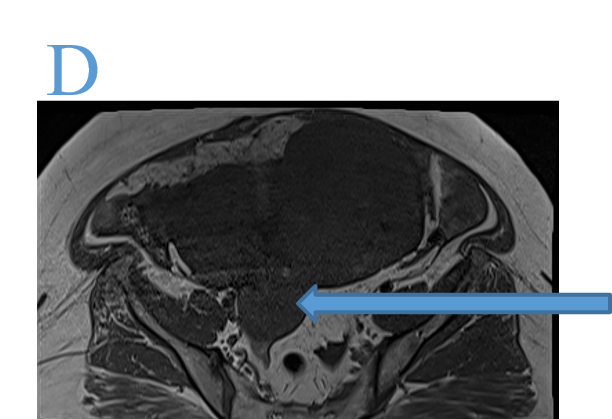
- A large, relatively well-defined, lobulated T2 hypointense non diffusion restricting solid lesion with smooth contours in the pelvis in the midline arising from right ovary. Superiorly the lesion is seen extending upto the level of L4 vertebral body. Anteriorly the lesion is seen abutting the anterior abdominal wall (left rectus abdominis muscle).
- No post contrast enhancement.
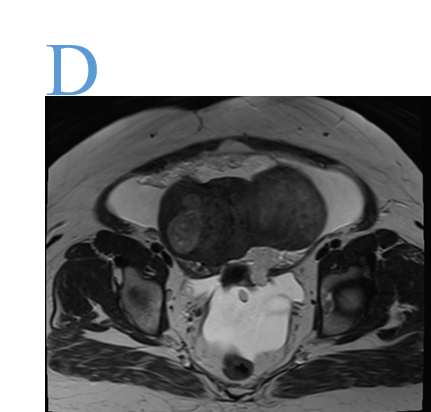
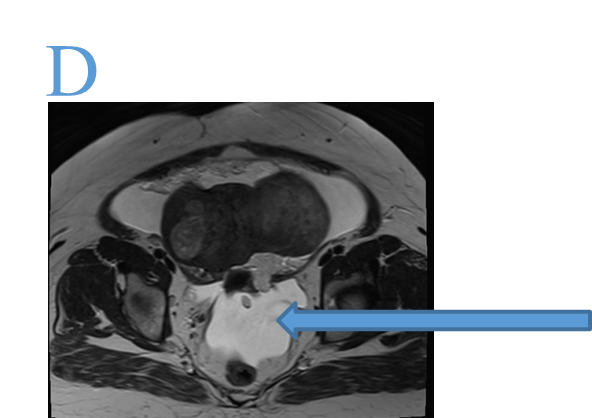
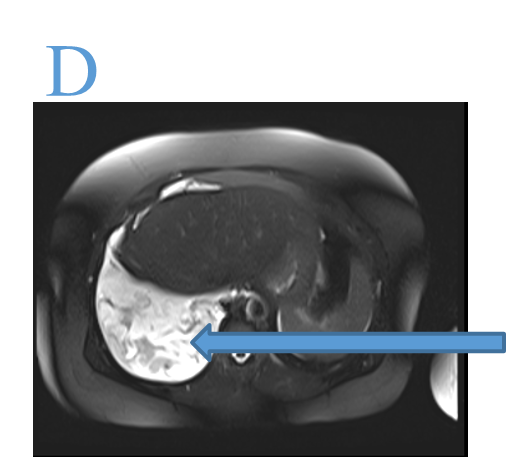
- A cystic lesion with thin internal septations, which is hyperintense on T2, hypointense on T1 arising from the right ovary.
- Mild to Moderate ascites.
- Gross right pleural effusion underlying passive atelectasis of the right lung.
DIAGNOSIS:
- Pleural fluid - exudative lymphocyte predominant with no malignant cells. AFB, ADA was negative.
- CEA- 0.6,CA 19-9 - 4.9, CA-125 - 452.
- Meigs syndrome.
DISCUSSION:
- Meigs syndrome is characterized by benign ovarian tumors that present with ascites and pleural effusions.
- It commonly affects postmenopausal women; however, when identified in younger individuals, consider Gorlin syndrome, a familial cancer syndrome.
Pathophysiology
- Pleural effusions in Meigs syndrome have been hypothesized to be secondary to the passage of ascitic fluid to the pleural space through the diaphragm or diaphragmatic lymph nodes.
Mechanisms for pathophysiology of ascites
- fluid leakage from edematous fibromas.
- tumor pressure on pelvic and abdominal lymphatics.
- lymphatic blockage.
Vascular endothelial growth factor that raises capillary permeability has also been associated with the development and accumulation of pleural and peritoneal fluid.
Benign tumours associated with Meigs syndrome include.
- Fibromas
- Thecomas
- Brenner tumours
- Granulosa cell tumours
Although typically associated with ovarian malignancy, elevated serum CA-125 levels have been noted in some cases of Meigs syndrome.
Therefore, patients with elevated CA-125 levels and adnexal mass are often misdiagnosed as having ovarian malignancy.
Diagnostic Imaging:
- Pelvic and abdominal ultrasonography.
- A chest x-ray - for pleural effusions and any pulmonary nodules suspicious of malignancy.
- Computed tomography (CT) of the chest, abdomen, and pelvis -exclude differential diagnoses of ascites, such as metastases, masses originating from the gastrointestinal tract, pulmonary lesions, and liver cirrhosis.
- Positron emission tomography (PET)/CT - confirm the benign nature of the ovarian mass and determine whether other malignant lesions are present.
Fluid Analysis and Cytology –
- In most patients with Meigs syndrome, the pleural fluid is exudative with no malignant cells.
- Tuberculosis Screening.
The definitive diagnosis of Meigs syndrome can only be made once a tissue sample has been obtained and the etiology of the ovarian mass has been identified. Therefore, the exclusion of differential diagnoses is essential before definitive surgical planning.
References:
- Mohammed SA, Kumar A, Cue L. Meigs Syndrome. [Updated 2024 Jul 27].
- In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
- Available from: https://www.ncbi.nlm.nih.gov/books/NBK559322/
Dr MADHU KUMAR SB
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr SHIKHA JOSHI
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
