
24 year young lady presented with complains of severe abdominal pain predominantly in the lower abdomen. Known case of uterine fibroids. Recently diagnosed with diabetes.
FINDINGS
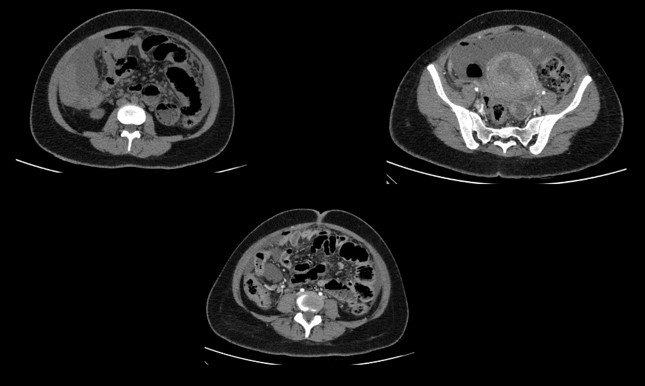
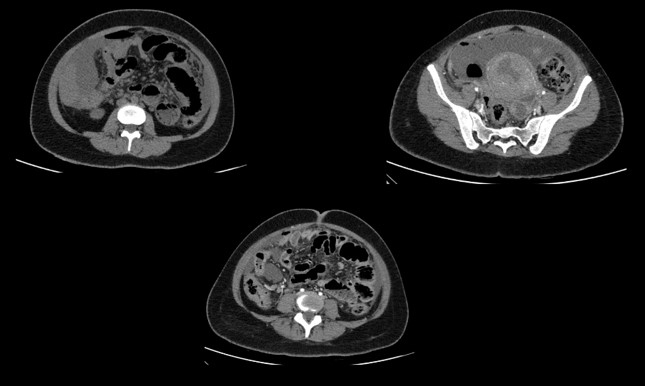
CECT ABDOMEN AND PELVIS - DAY 1
LEGENDS
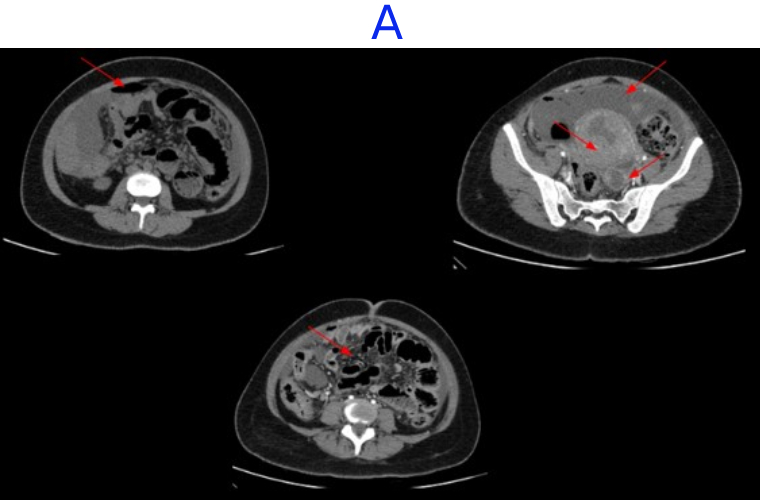
- A. Mild pneumoperitoneum. Few heterogeneously enhancing fibroids seen. Tubular hypodense area in left adnexa - likely pyosalpinx Diffuse greater omental fat stranding and peritoneal thickening - suggestive of peritonitis.
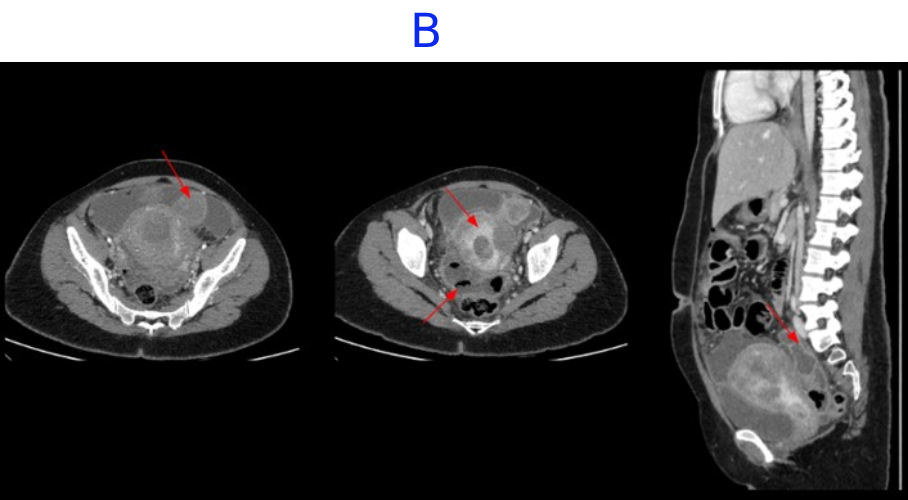
- B. Tubular hypodense area in left adnexa - likely pyosalpinx. Subserosal fibroid in upper corpus.Few loculated fluid pockets with air foci are seen in the pouch of douglas
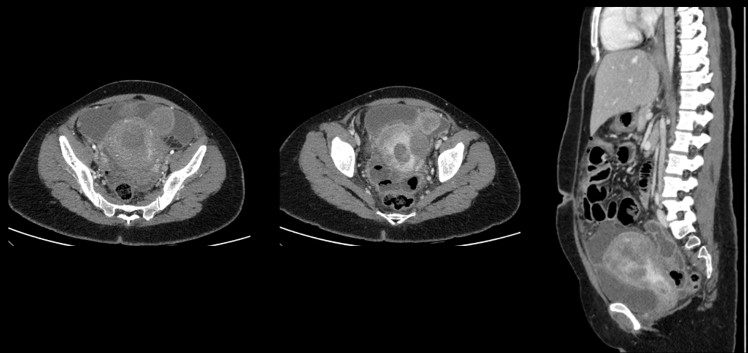
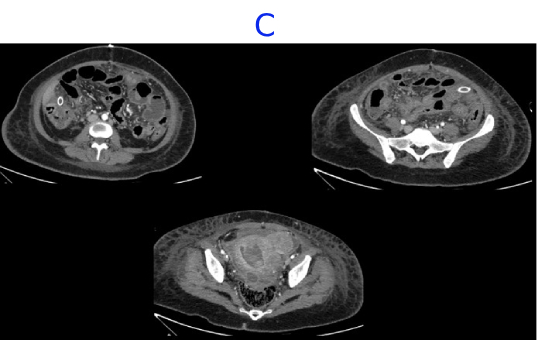
- C. CECT ABDOMEN AND PELVIS- DAY 7- STATUS POST EXPLORATORY LAPAROTOMY AND PERITONEAL LAVAGE
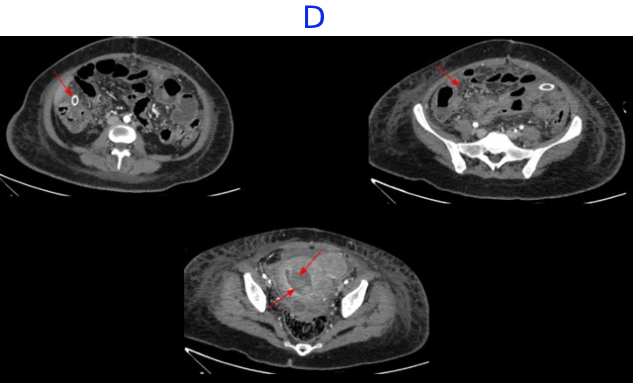
- D. Bulky uterus with a hypodense submucosal lesion protruding into the endometrial cavity from the fundus showing heterogeneous enhancement - infected vs infarcted fibroid. Abnormally enhancing endometrial lining with hypodense content within the endometrial cavity - possible endometritis with pyometra. Pelvic peritonitis with residual trace fluid in the pelvis. Interval resolution of pneumoperitoneum. Abdominal drains in situ.
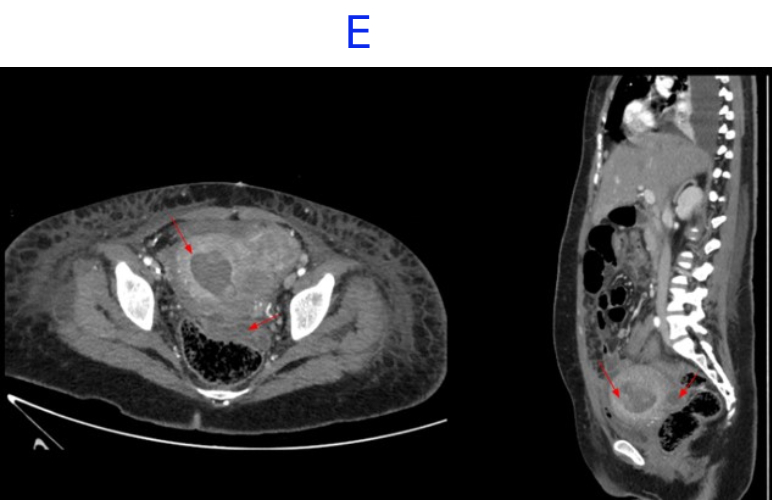
- E. Bulky uterus with a hypodense submucosal lesion protruding into the endometrial cavity from the fundus showing heterogeneous enhancement - infected vs infarcted fibroid. Abnormally enhancing endometrial lining with hypodense content within the endometrial cavity - possible endometritis with pyometra. Left sided pyosalpinx.
- Bulky uterus with a hypodense submucosal lesion protruding into the endometrial cavity from the fundus showing heterogeneous enhancement - infected vs infarcted fibroid.
- Abnormally enhancing endometrial lining with hypodense content within the endometrial cavity - possible endometritis with pyometra
- Left sided hydro/pyosalpinx.
PYOMYOMA
- Large uterine leiomyoma following necrosis with superimposed infection results in the condition known as pyomyoma.
- Gradual increase in size will make the leiomyoma outgrow its blood supply. This in turn leads to different types of degeneration namely hyaline, myxoid, cystic, or red degeneration.
- Second, exophytic subserosal leiomyoma which project into the abdominal cavity can become pedunculated and undergo torsion resulting in infarction.
- Red or carneous degeneration and uterine artery embolization associated degeneration results from venous thrombosis along the periphery of a leiomyoma leading to infarction.
- On USG- a painful myoma with changes in the echogenicity suggesting internal cystic lesions can suggest red degeneration and infarction.
- Myomas with red degeneration are characterized by acute onset abdominal pain, mild fever, localized tenderness over the myoma and leukocytosis. They can become infected and turn to pyomyomas. Extensive necrotic areas can become infected with anaerobic bacteria.
- MRI should be considered in such situations to confirm the diagnosis. Pyomyomas usually lead to inflammatory changes and tissue necrosis, arising suspicion due to the low ADC on MRI.
- Patients with a history of myomatosis who develop sepsis with unidentifiable foci should be suspected for pyomyoma.
KEY POINT
The differential diagnosis of a pelvic mass with a clinical presentation suggestive of infection includes endometritis, pyometra, tubo-ovarian abscess, complicated gynecological neoplasm, and pyomyoma.
A pyomyoma is a rare but potentially fatal condition resulting from infarction and infection of a leiomyoma through bacterial seeding and direct, hematogenous, or lymphatic dissemination.
Because of the rarity of pyomyomas, low clinical suspicion delays its diagnosis and predisposes patients to possible complications, such as purulent peritonitis or sepsis.
MANAGEMENT
Laparotomy with peritoneal lavage. Vaginal drainage of endometrial collection with laparotomy with myomectomy + bilateral salpingectomy
REFERENCES
Magnetic resonance imaging findings of spontaneous pyomyoma in a premenopausal woman managed with myomectomy: A case report
David Martínez Gustavo E Sanche, Jhonatan Gómez , Luis J Sonda Luis D Suárez , Carlos S López Juan J Vega Daniel A Cepeda
2023 Mar 28;15(3):83–88. doi: 10.4329/wjr.v15.i3.83
Ascending infection causing pyomyoma in a young woman Avantika Gupta, Madhavi Mathur Gupta, Usha Manaktala
Dr MADHU KUMAR S B
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr NIKITHA U N
Radiology Resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
