
51 yr old male presented with abnormal behaviour.
- 51 yr old male presented with abnormal behaviour.
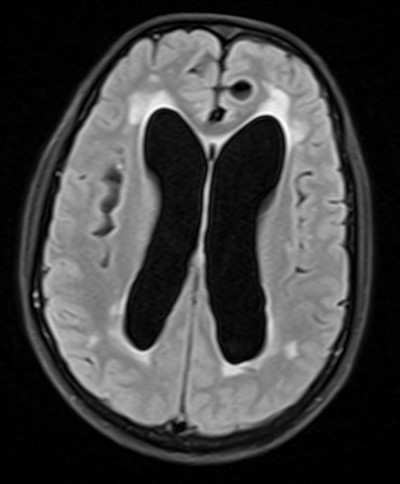
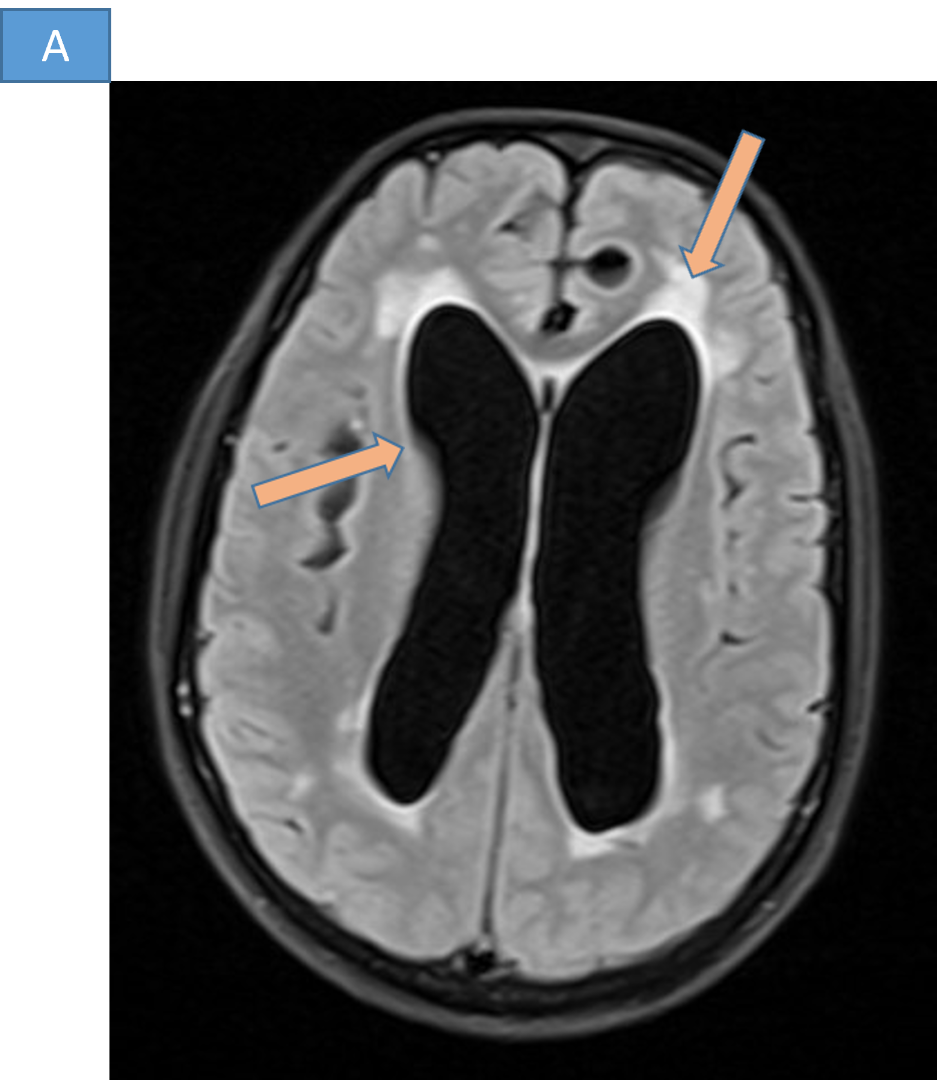
- A. Hydrocephalus with transependymal seepage of CSF.
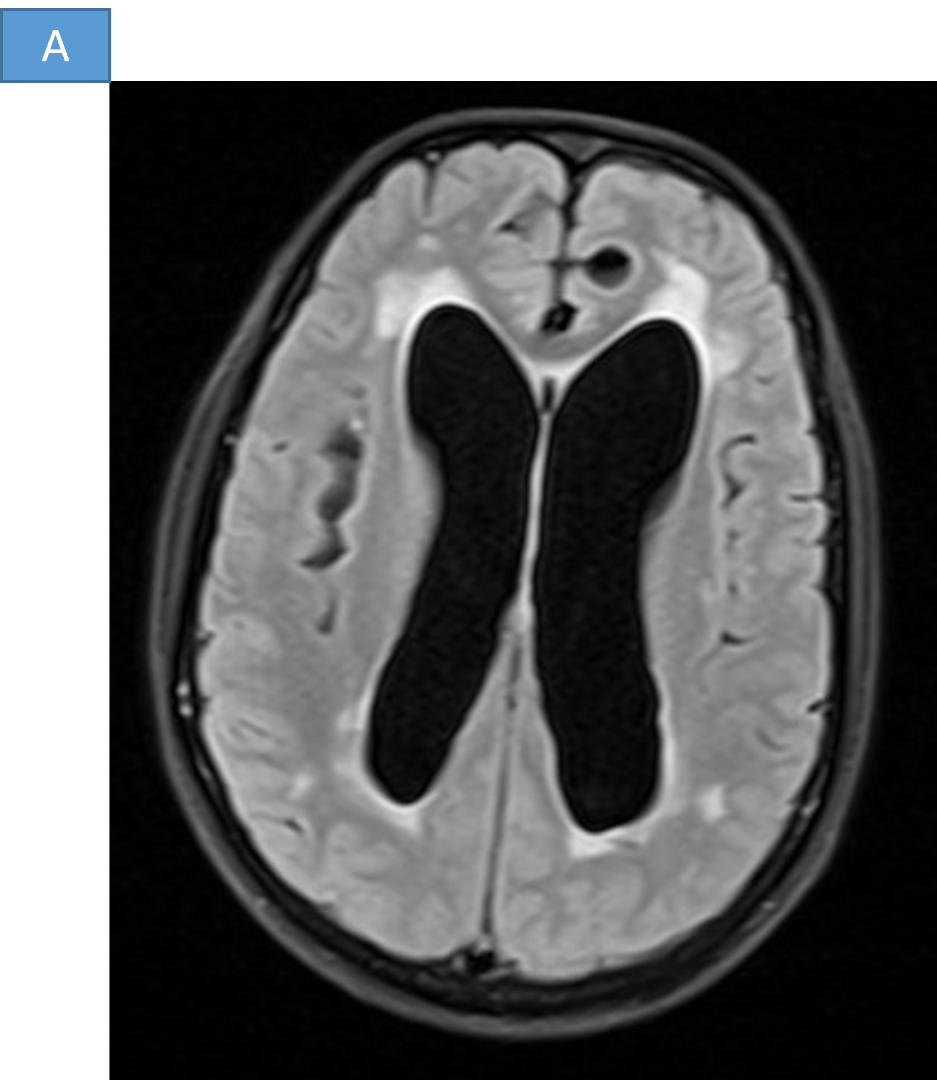
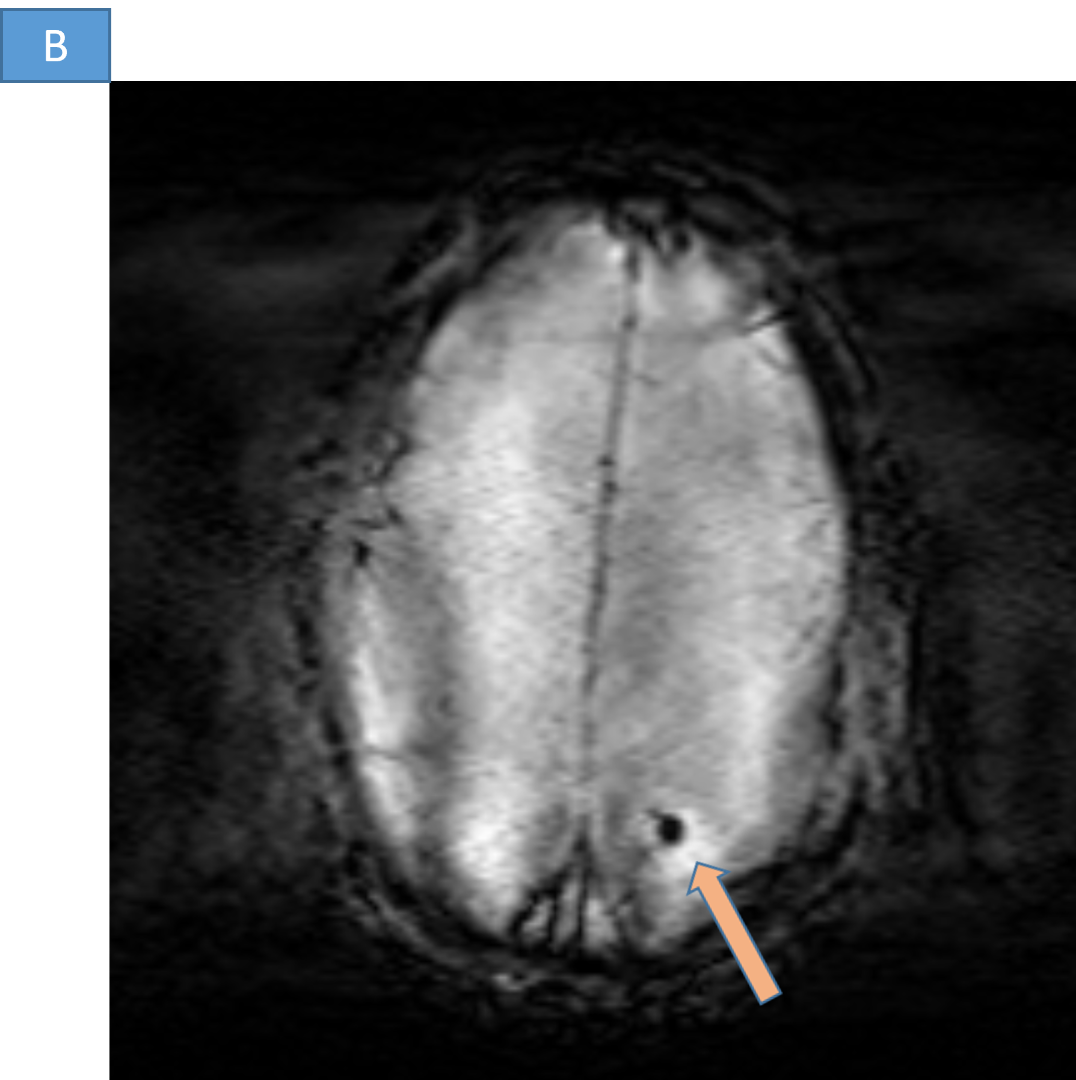
- B. Parenchymal calcification.
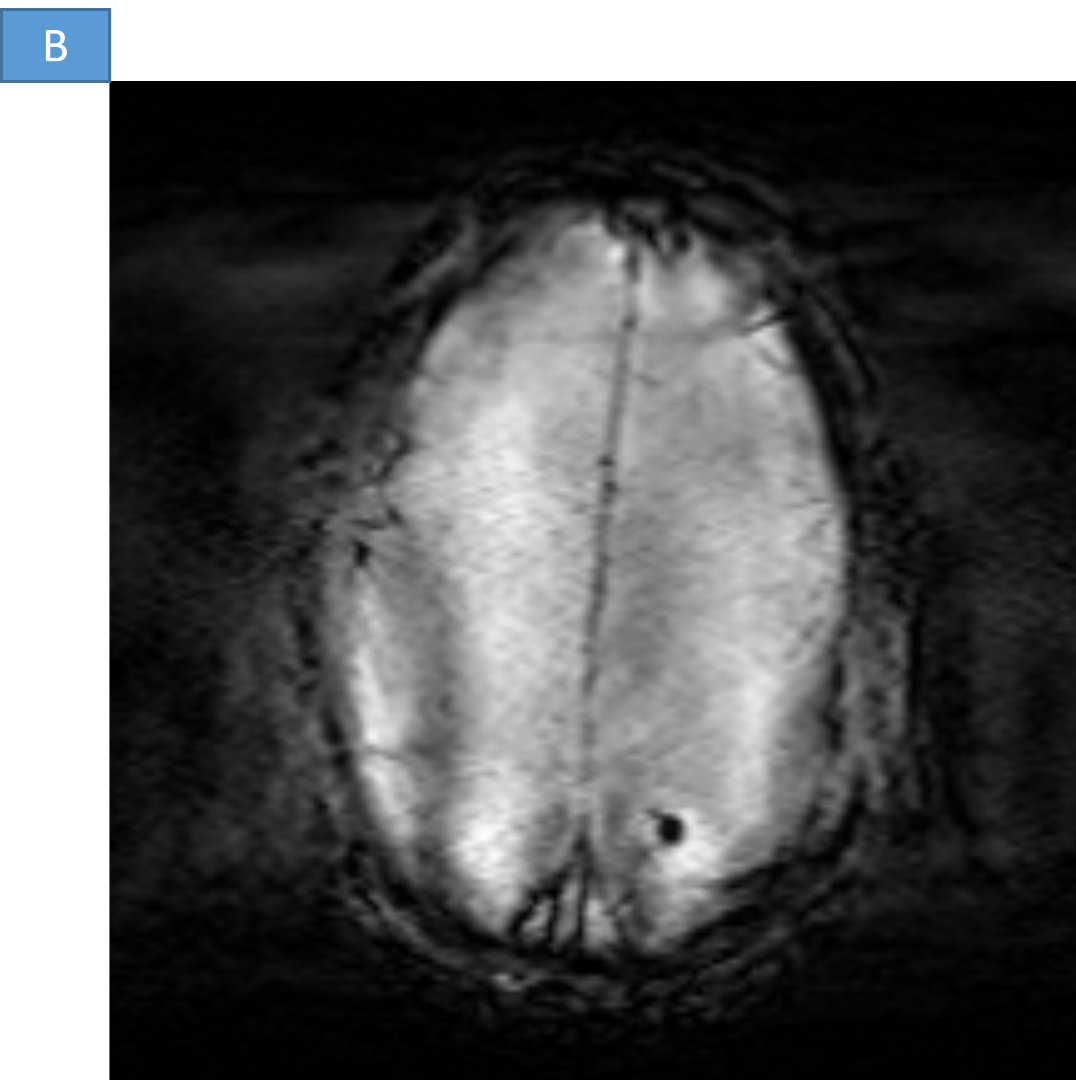
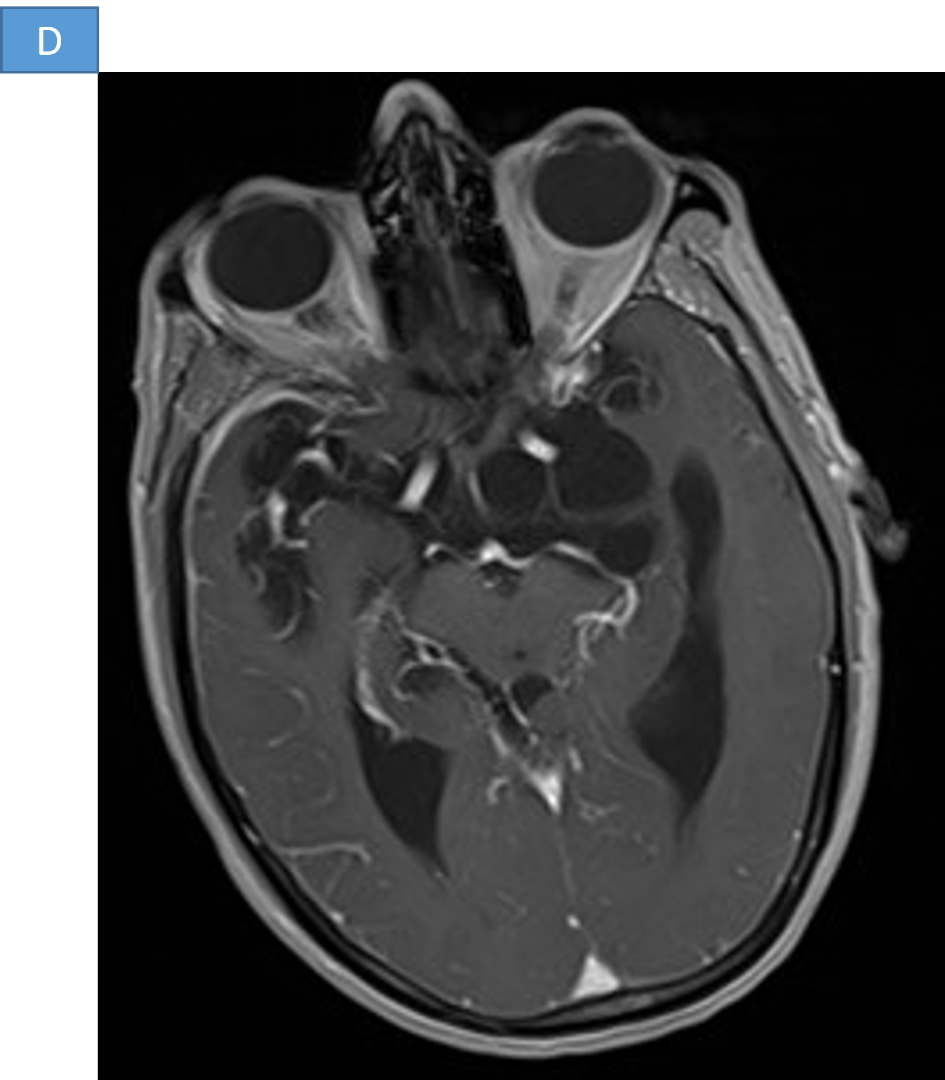
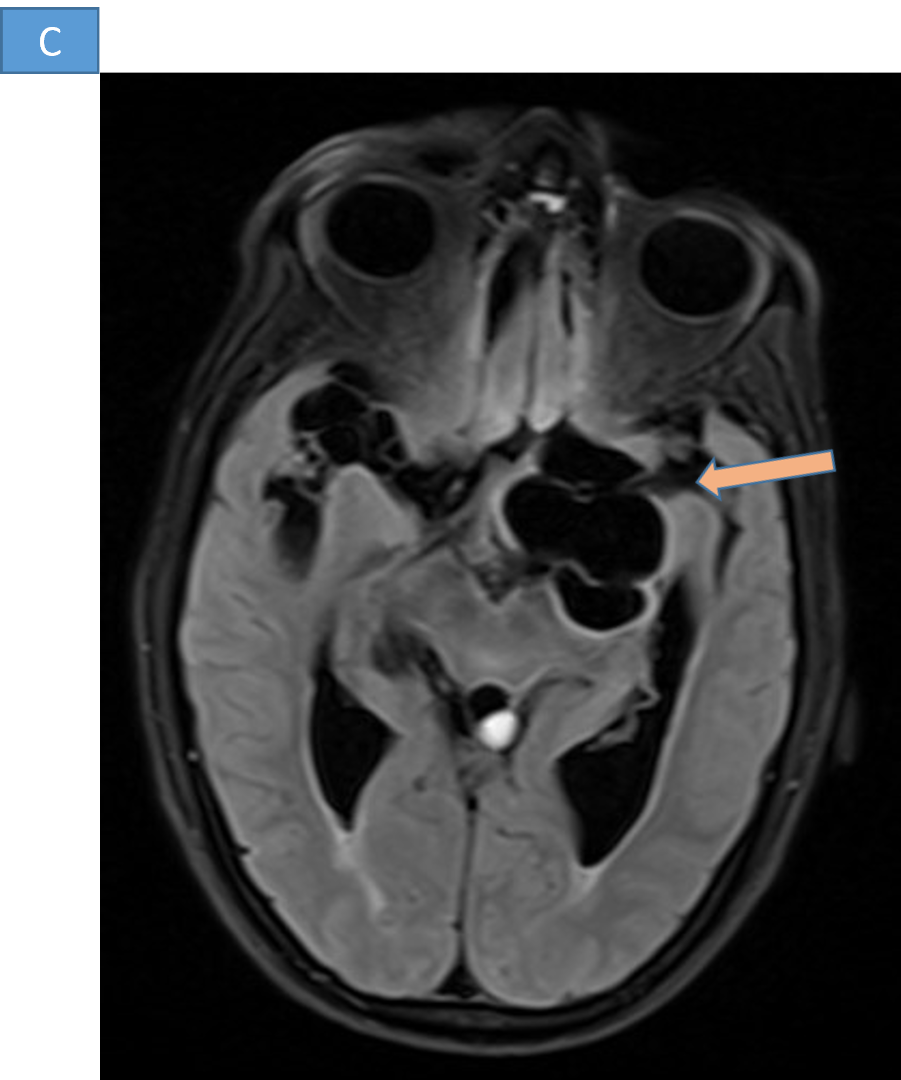
- C and D. Multiple multiloculated CSF intensity lesions in bilateral sylvian fissures and suprasellar cisterns with no post contrast enhancement.
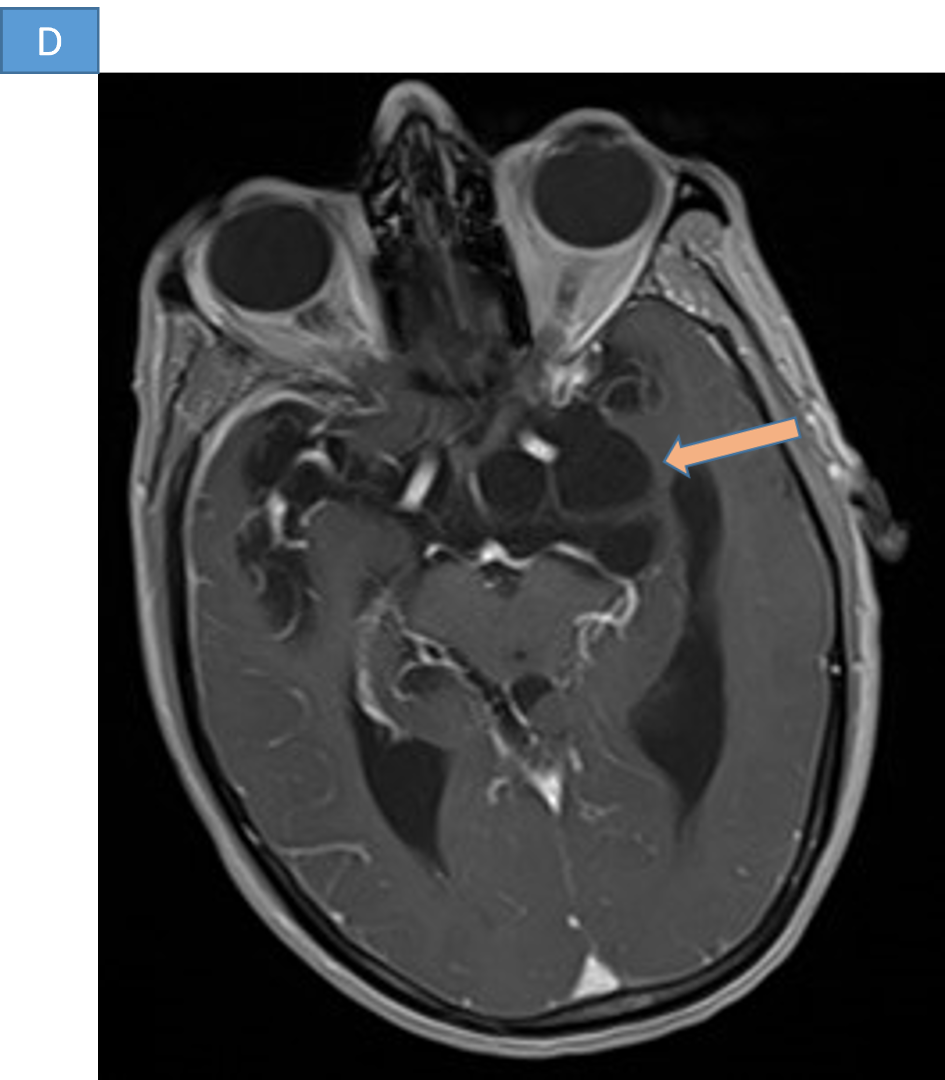
RACEMOSE NEUROCYSTCERCOSIS
DISCUSSION
Racemose neurocysticercosis
- Invasive parasitic infection of the central nervous system caused by the larval stage of the tapeworm Taenia solium.
- Most frequent cause of acquired epilepsy in the developing countries.
- Parasitic infestation is endemic to South and Central America, Southeast Asia, China, and Sub-Saharan Africa.
- Depending on the site of involvement, they are classified into intraparenchymal, extra parenchymal (subarachnoid-cisternal, meningeal, intraventricular) and mixed types.
- The racemose variant of extraparenchymal NCC is characterized by the presence of multilobulated confluent cysts within the basal subarachnoid space that appear “grape-like” both radiographically and pathologically.
- Clinical presentation can be variable.
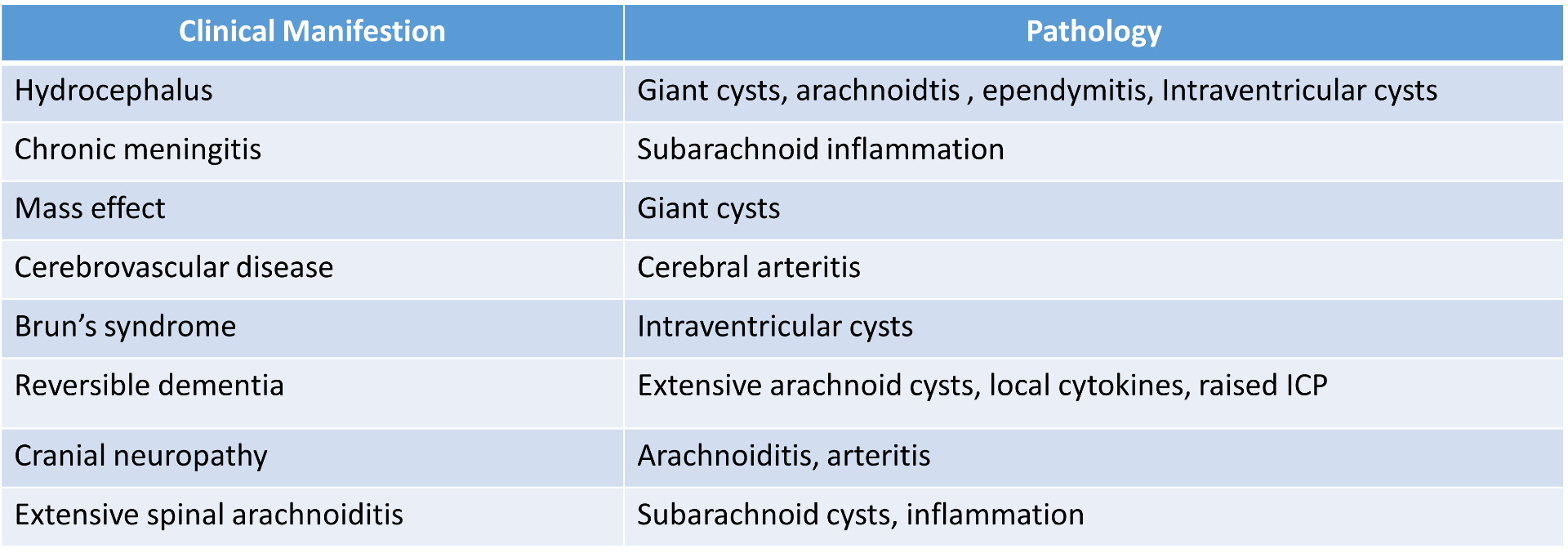
Clinical manifestations of Racemose NCC
RADIOLOGICAL INVESTIGATIONS
Computed tomography (CT)
- Sensitivity and specificity of more than 95% in the diagnosis of the parenchymatous form of neurocysticercosis.
- Lower sensitivity and specificity for diagnosing the ventricular and cisternal forms.
- Helpful in detecting calcifications.
MRI
- The cisternal or ventricular forms of neurocysticercosis are readily visualized in MRI.
- The cysts are usually larger than in the parenchymal forms and have a multilocular appearance, tend to displace neighboring structures, and behave as lesions with a mass effect.
- The signal intensity is similar to that of the cerebrospinal fluid.
- Normally do not show significant contrast enhancement; may show peripheral enhancement
- Cysticerci usually do not contain scolices. If a scolex is seen, it is almost diagnostic/pathognomonic.
- Conventional MR sequences such as T1- and T2-weighted images and fluid-attenuated inversion recovery images may miss intraventricular/cisternal neurocysticercosis cysts.
- Three-dimensional (3D), very heavily T2-weighted sequences, such as constructive interference in steady state or fast imaging employing steady-state acquisition, are good sequences for evaluating intraventricular cysts.
- Another MR sequence that is also useful is the 3D spoiled gradient recalled echo sequence, which provides T1 information.
DIFFERENTIAL DIAGNOSIS
- Arachnoid cysts
- Porencephaly
- Hydatid disease
- Cystic astrocytoma
- Colloid cyst of third ventricle
Diagnosis
- Positive hydatid serology will further be supporting evidence.
- Serological tests (enzyme-linked immunoelectrotransfer blot assay, enzyme-linked immunosorbent assay) that detect anticysticercal antibodies in serum or CSF inherently lack specificity or sensitivity, thereby precluding their reliability in isolation.
- MRI is the primary diagnostic modality used for the detection of cysticercus lesions and their secondary complications.
Treatment
- Medical management with cysticidal agents, corticosteroids, and antiepileptic drugs
- Surgical management to remove the cyst or to insert a shunt to treat hydrocephalus.
REFERENCES
- Mahale RR, Mehta A, Rangasetty S. Extraparenchymal (Racemose) Neurocysticercosis and Its Multitude Manifestations: A Comprehensive Review. J Clin Neurol. 2015 Jul;11(3):203-211. https://doi.org/10.3988/jcn.2015.11.3.203
- Sharma S, Singh A, Mani VE, Mishra SC, Chaturvedi P, Jain S, Kumar S, Jain N. Racemose neurocysticercosis: a case series. BJR Case Rep. 2024 Jan 19;10(1):uaae001. doi: 10.1093/bjrcr/uaae001. PMID: 38352260; PMCID: PMC10860505.
- Krupa K, Krupa K, Pisculli ML, Athas DM, Farrell CJ. Racemose neurocysticercosis. Surg Neurol Int. 2016 Feb 5;7:12. doi: 10.4103/2152-7806.175881. PMID: 26958418; PMCID: PMC4766808.
- https://www.ajnr.org/ajnr-case-collections-diagnosis/racemose-neurocysticercosis.
Dr. HARSHA CHADAGA
SENIOR CONSULTANT RADIOLOGIST AND HOD OF RADIOLOGY
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU
Dr. VINEETH BABY
FELLOW IN CROSS SECTIONAL IMAGING
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU
