37 year old male patient with sudden onset headache and nausea. Past history: Old trauma 2 weeks back.
On examination:
- His neurological examination revealed papilledema and features of raised intracranial pressure.
- GCS: 15/15
- No focal neurological deficit.


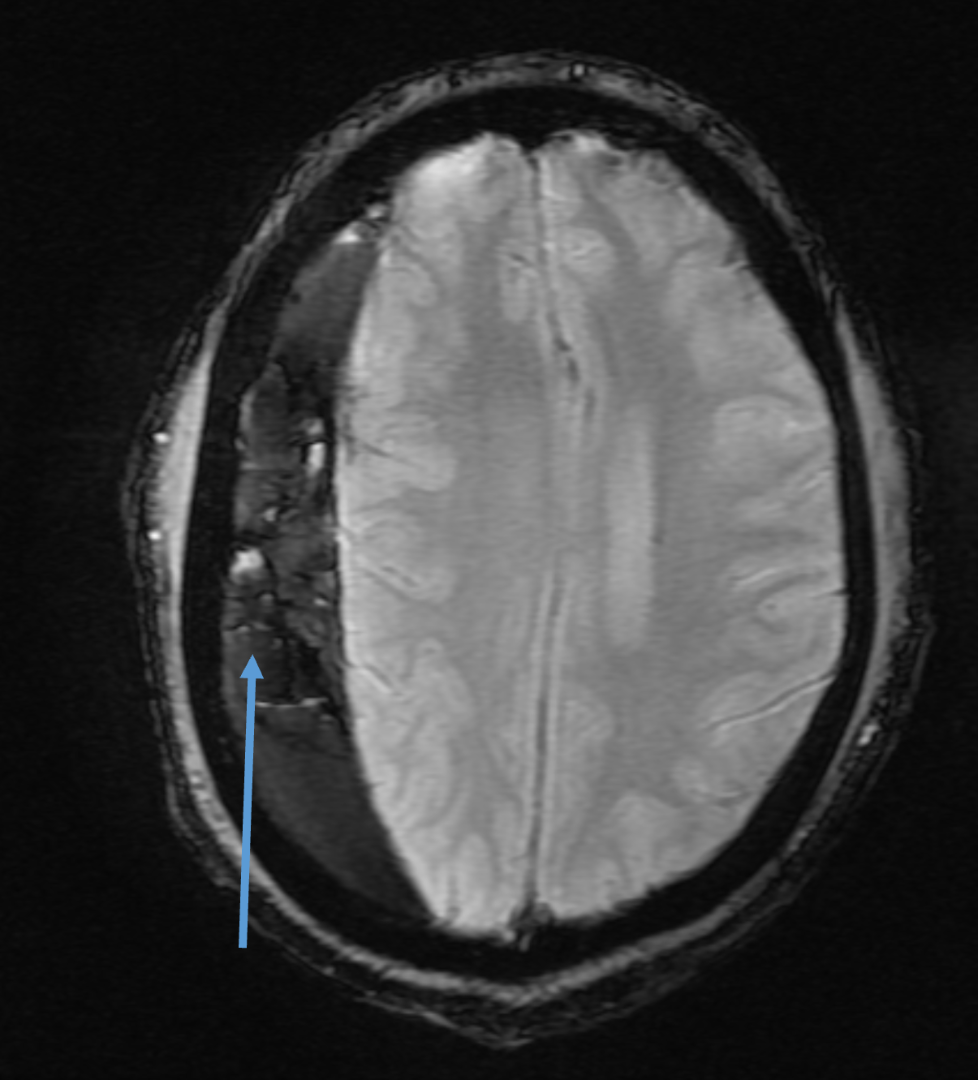
A.
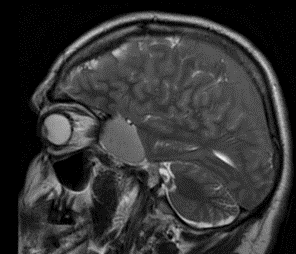
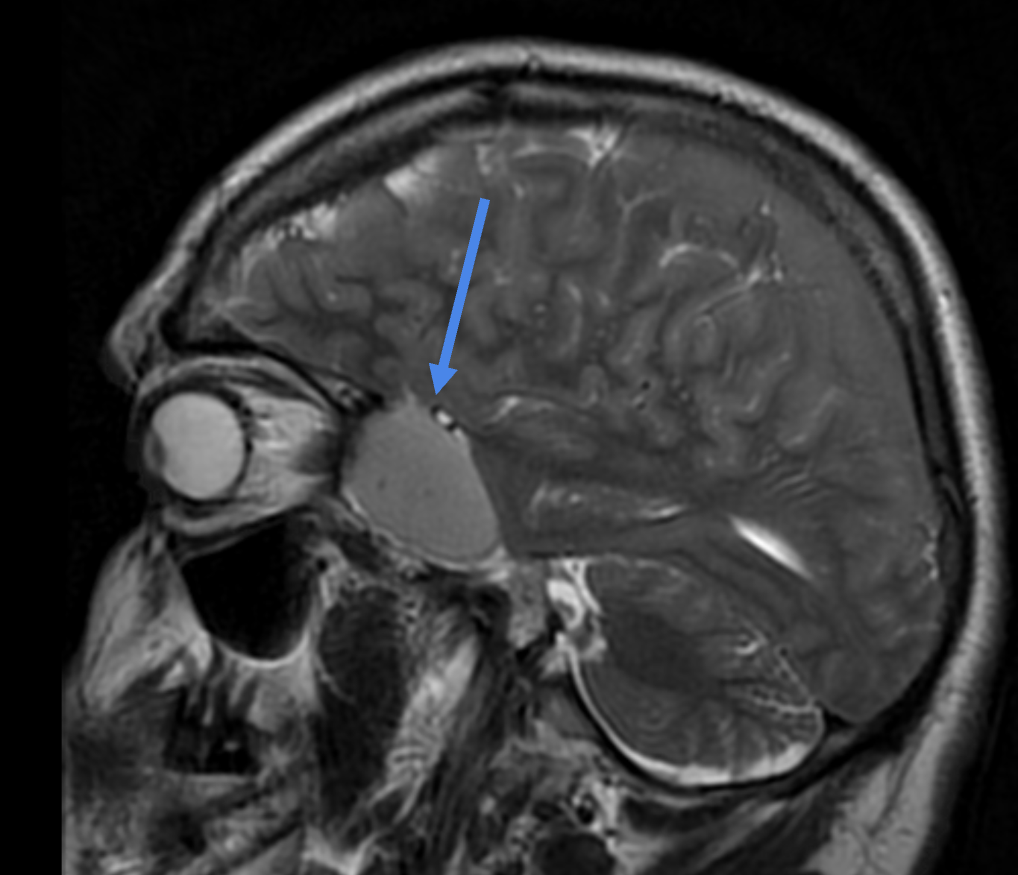
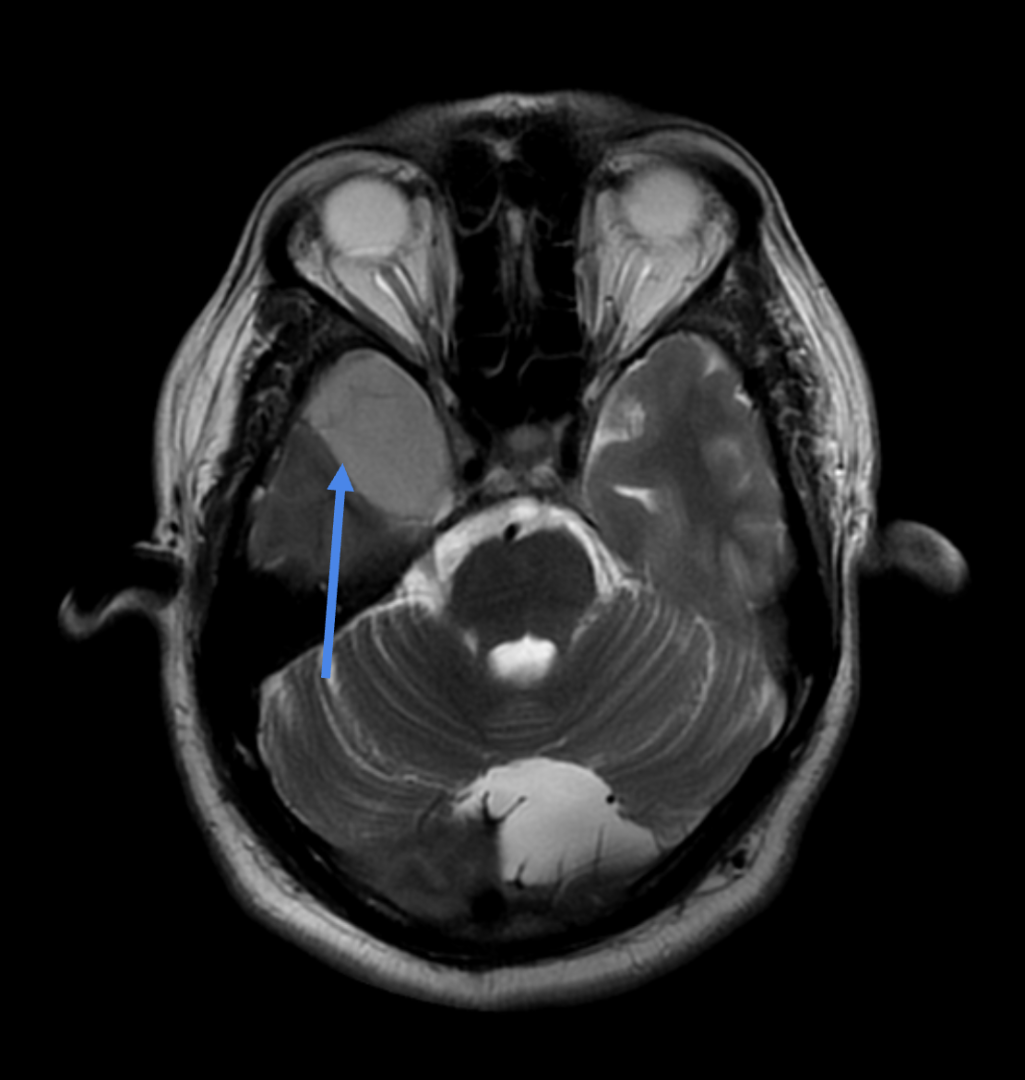
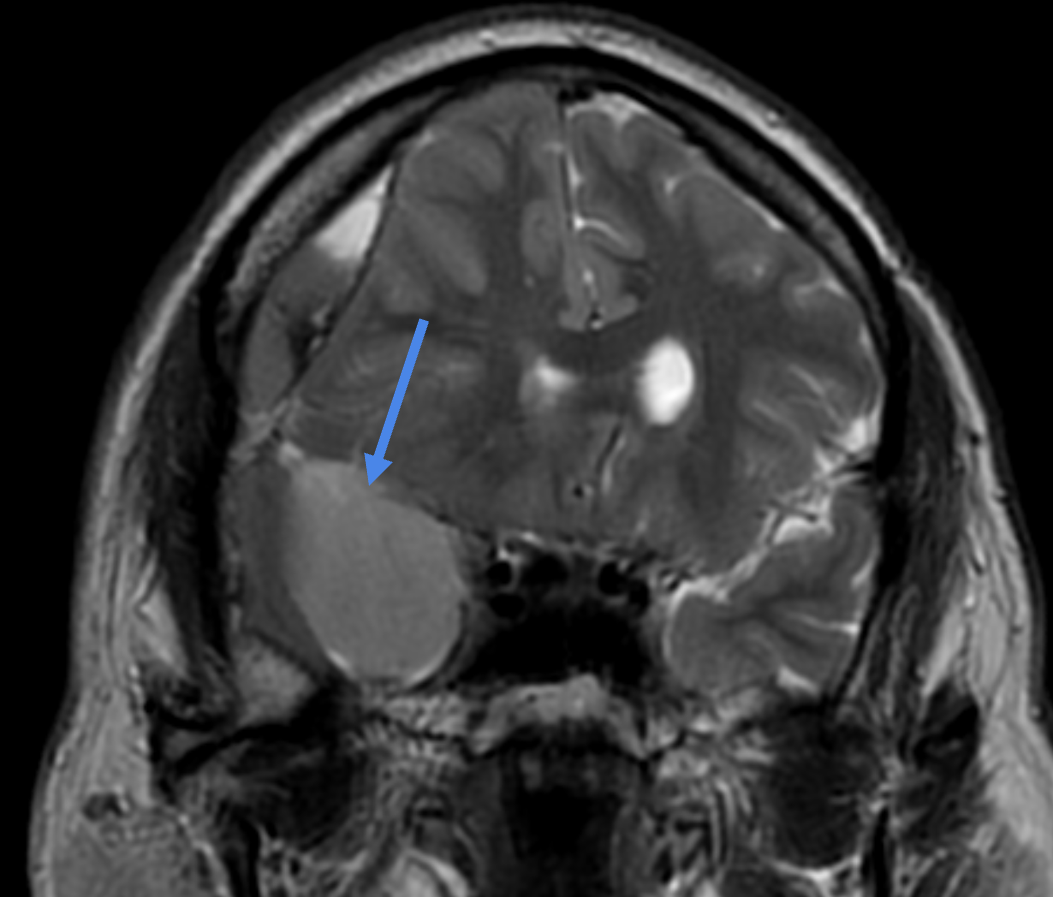
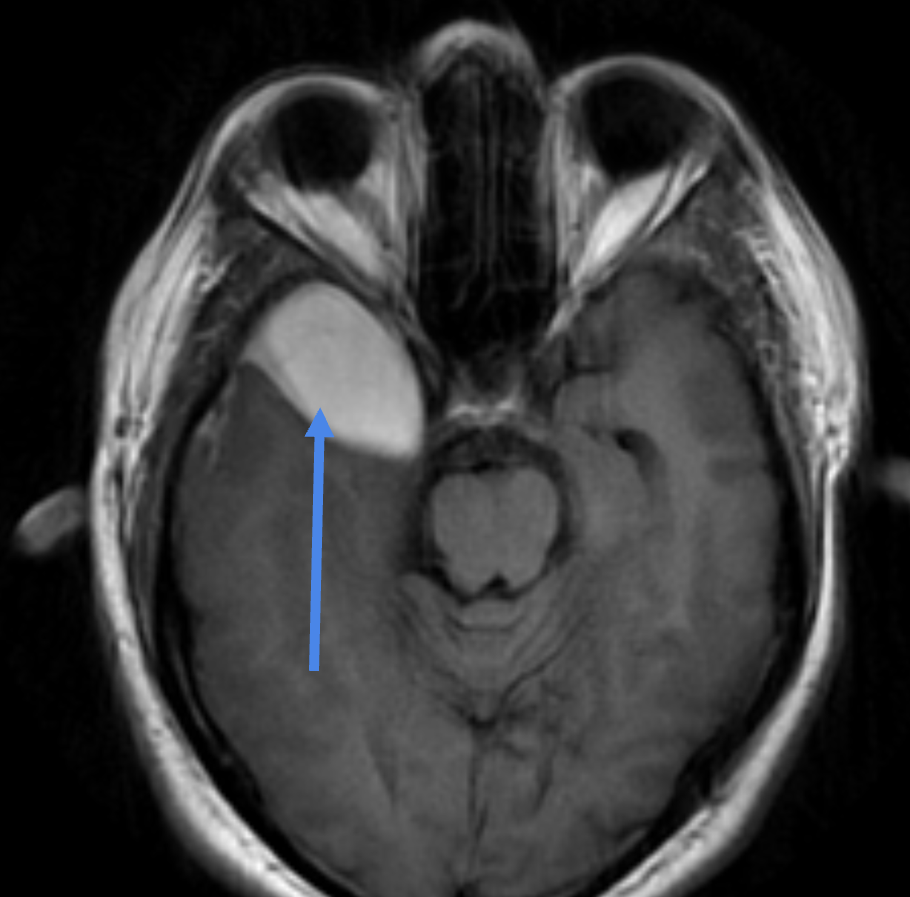
- A well defined extra-axial T1 and T2 hyperintense lesion measuring 4.1 x 2.7 cm is seen anterior to the right temporal lobe mildly effacing the right anterior temporal lobe.
- Along the posterolateral aspect on right side there extension of the contents into the subdural space forming a large subdural collection.
- Rest of the cerebral hemispheres show normal morphology and T1, T2 signal characteristics.
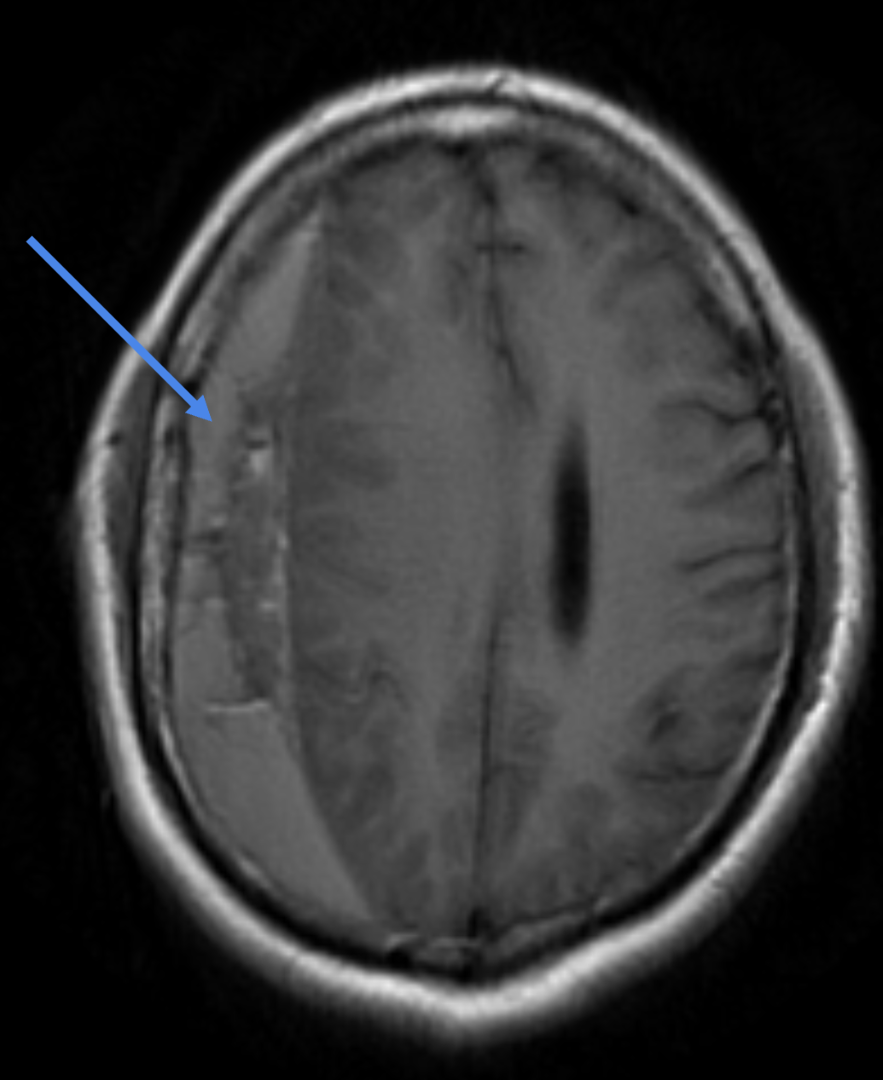
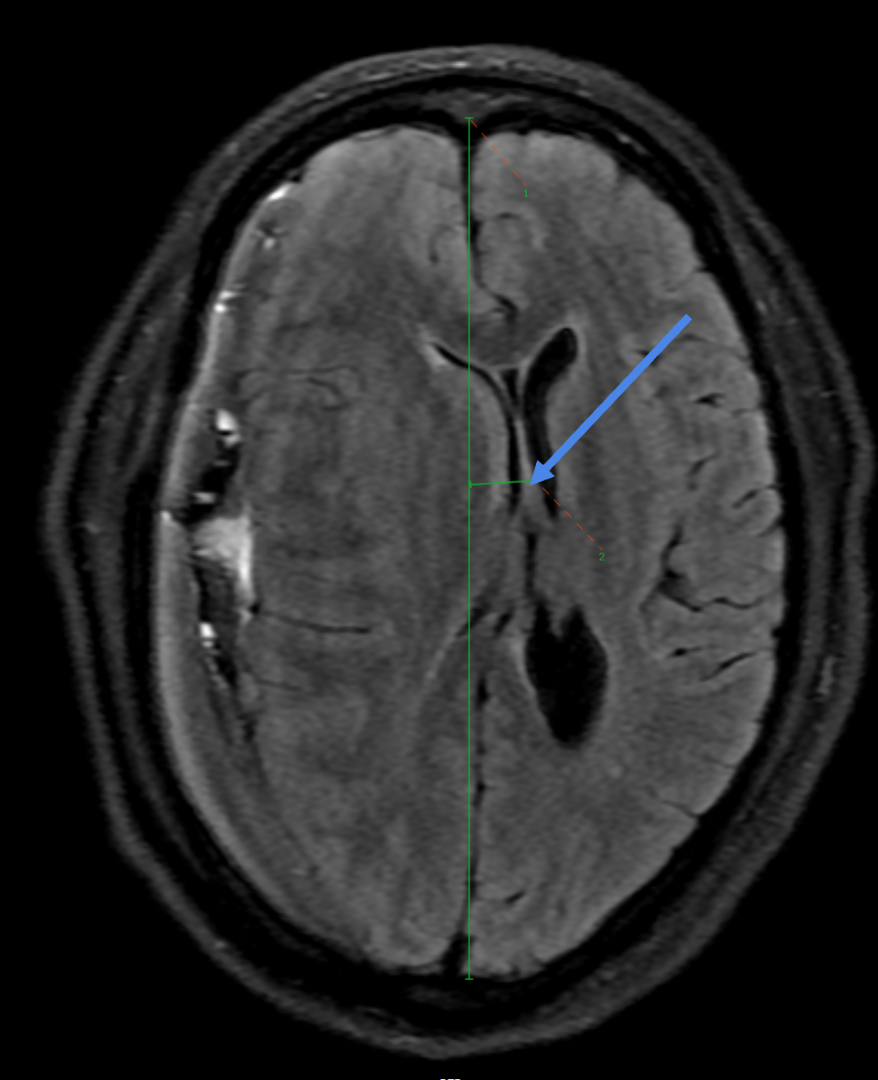
B.
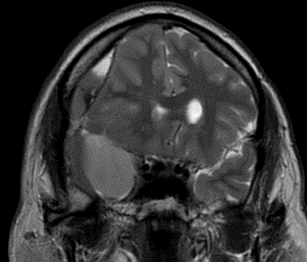
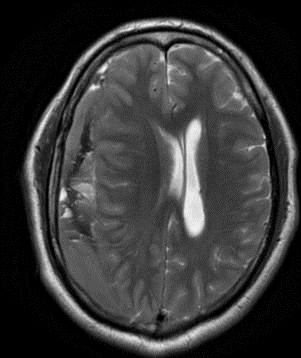
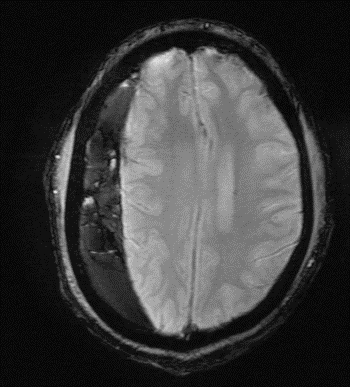
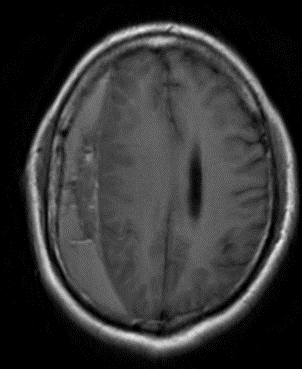
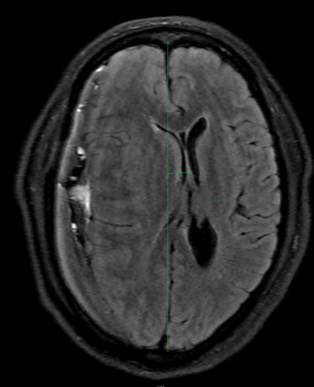
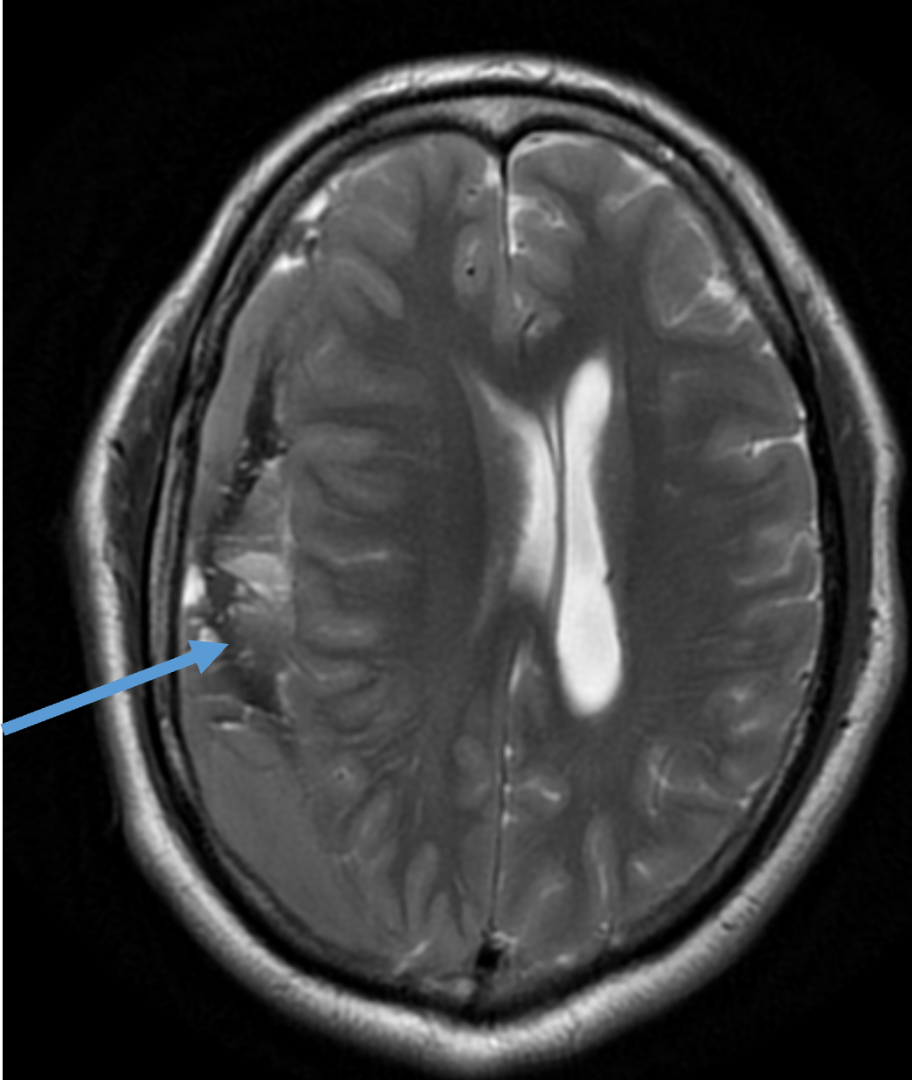
- A large late subacute subdural haemorrhage is seen along the entire right cerebral convexity with maximum thickness measuring 2.1 cm is seen.
- Mass effect is seen in the form of locoregional sulcal effacement and compression of right lateral and third ventricles with midline shift to the left measuring 1.3 cm.
DIAGNOSIS
- A well defined extra-axial T1 and T2 hyperintense lesion anterior to the right temporal lobe with extension into the subdural space forming a large subdural collection.
- A large late subacute subdural haemorrhage is seen along the entire right cerebral convexity with mass effect and midline shift as described.
Features likely to represent right anterior temporal extra axial arachnoid cyst with rupture and associated right cerebral convexity subdural hemorrhage as described above.
DISCUSSION
Arachnoid cysts (ACs) are collections of cerebrospinal fluid that are thought to have a congenital origin and are encircled by an arachnoid sheet. These are rare cystic lesions, accounting for one percent of all intracranial masses. [1]
The sylvian fissure/middle cranial fossa is common location to nearly half of intracranial arachnoid cysts . About 60–80% of arachnoid cysts are found before the age of 15, primarily in the male population.[1]
Despite the fact that ACs typically have a stable volume, they can grow by a variety of methods , which can result in symptoms such intracranial pressure or direct compression of specific structures and exhibit signs of a ruptured cyst, which typically results in intracystic hemorrhage, subdural hematoma, or hygroma . Although minor head trauma is typically the cause of rupture, spontaneous rupture is sometimes possible.
It is uncommon for a middle fossa arachnoid cyst (MFAC) to spontaneously rupture. [1]
PATHOPHYSIOLOGY
Rupture could be caused by one of two causes. The first is a flap-valve mechanism that connects the cyst to the subarachnoid area as a result of a small head injury, allowing CSF to flow into the cyst from the subarachnoid space. As a result, the cyst enlarges and becomes more pressurized, eventually rupturing into the subdural space. [2]
Another postulate to the cause of bleeding is due to the rupture of an unsupported bridging veins that are stretched by the cyst and vulnerable to rupture by an increase in intracystic pressure . [3]
TREATMENT
Currently, fenestration of the cyst in the CSF spaces, either by craniotomy or utilizing the endoscopic approach, is the surgical option for managing arachnoid cysts. Nevertheless, none of the comparable examples documented in the literature employed the latter method. One viable option is to implant a cysto-peritoneal shunt.[1]
REFERENCES
- [1] Balestrino A, Piatelli G, Consales A, Cama A, Rossi A, Pacetti M, Fiaschi P, Pavanello M. (2020) Spontaneous rupture of middle fossa arachnoid cysts: surgical series from a single-center pediatric hospital and literature review. Child's Nervous System. 23:1-1. (PMID: 32206869)
- [2] Gelabert-González M, Fernández-Villa J, Cutrín-Prieto J, Allut AG, Martínez-Rumbo R. (2002) Arachnoid cyst rupture with subdural hygroma: report of three cases and literature review. Child's Nervous System. 1;18(11):609-13. (PMID: 12420120)
- [3] Offiah C, St Clair Forbes W, Thorne J.(2006) Non-haemorrhagic subdural collection complicating rupture of a middle cranial fossa arachnoid cyst. The British journal of radiology. 79(937):79-82. (PMID: 16421410)
Dr RAHUL KARTHIK L
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr M MATHEW JAMES
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.