25-year-old female with peri-umbilical abdominal pain and weight loss of 8kgs over a period of 1 year
- 25-year-old female with peri-umbilical abdominal pain and weight loss of 8kgs over a period of 1 year.
- Pain in the left upper arm and left chest and forearm since 2 weeks, aggravated on activities.
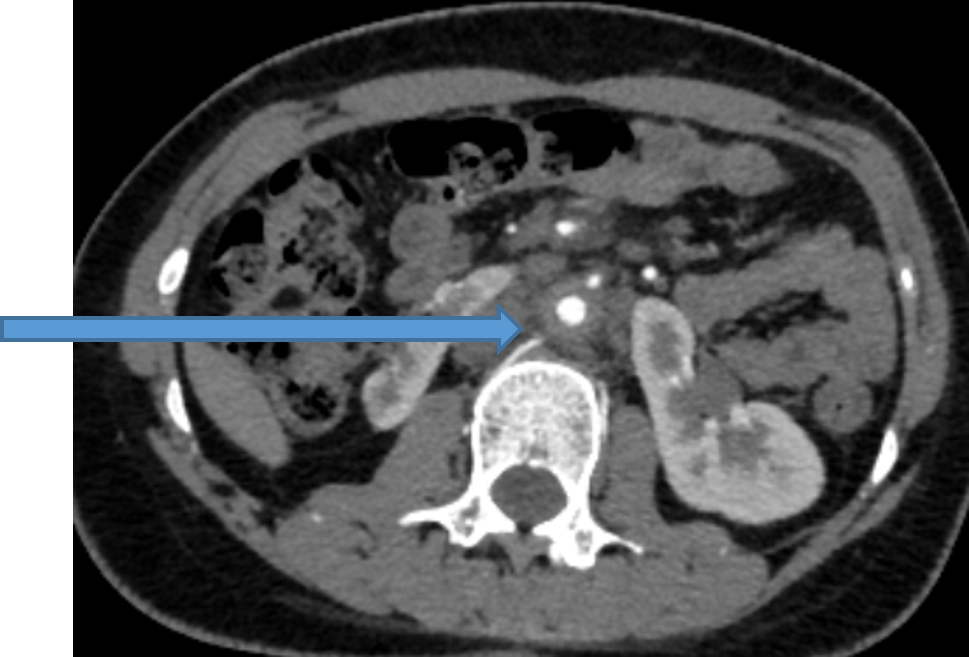

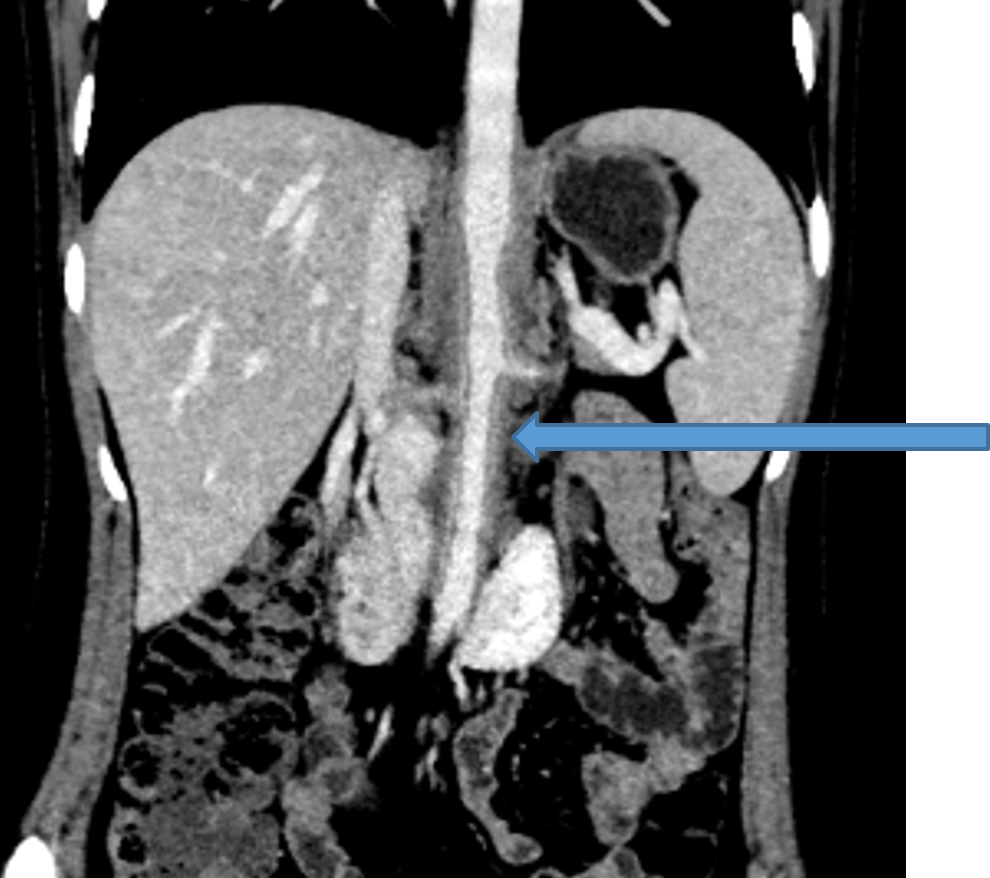

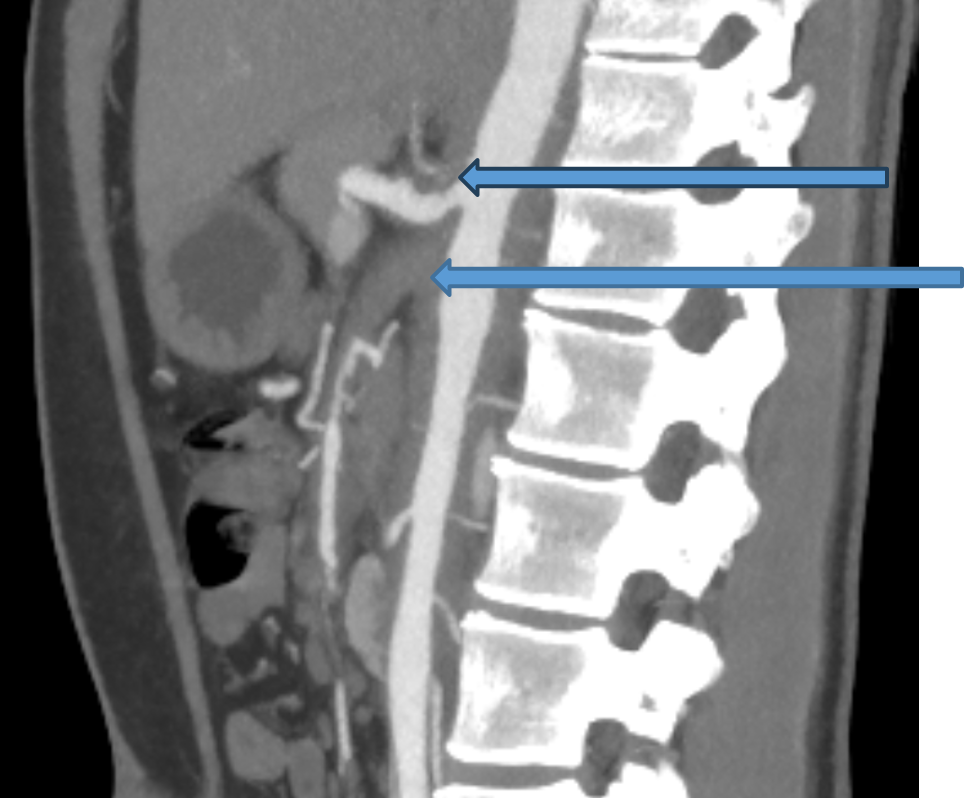



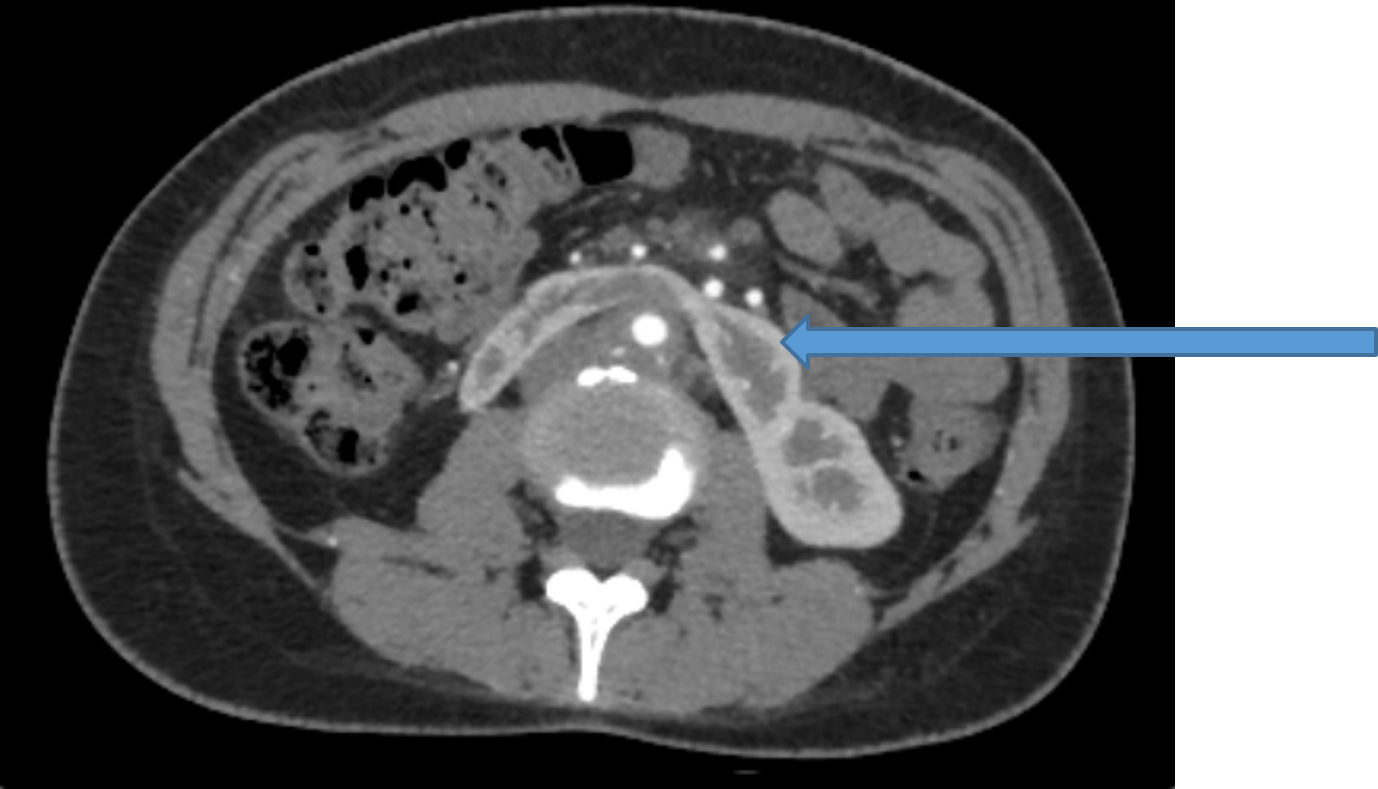
- Concentric uniform enhancing wall thickening of the abdominal aorta from the diaphragmatic hiatus extending upto the iliac bifurcation causing mild luminal narrowing.
- Mild narrowing of the celiac artery ostia; however, the branches of coeliac trunk appears normal.
- Concentric uniform wall thickening of proximal portion of superior mesenteric artery from its origin from aorta causing complete occlusion of arterial lumen. There is reformation of the superior mesenteric artery distally via collaterals from celiac artery.
- Concentric uniform wall thickening of both renal arteries causing moderate to severe luminal narrowing of the right renal artery lumen.
- Horseshoe configuration of kidneys. Right kidney appears atrophic. Left kidney appears mildly hypertrophied.
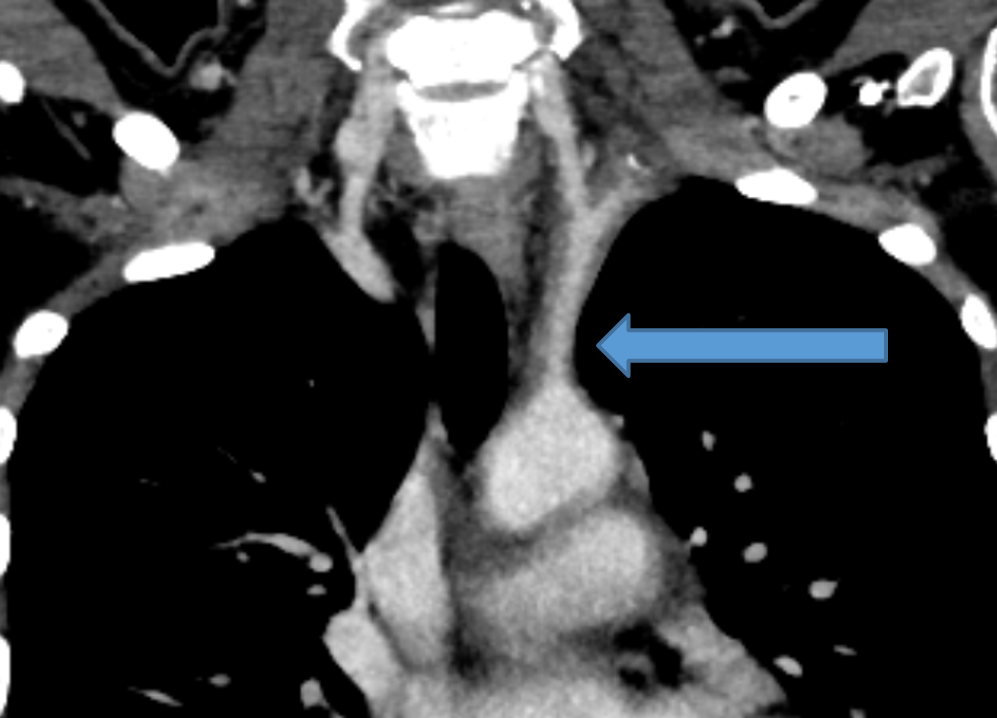
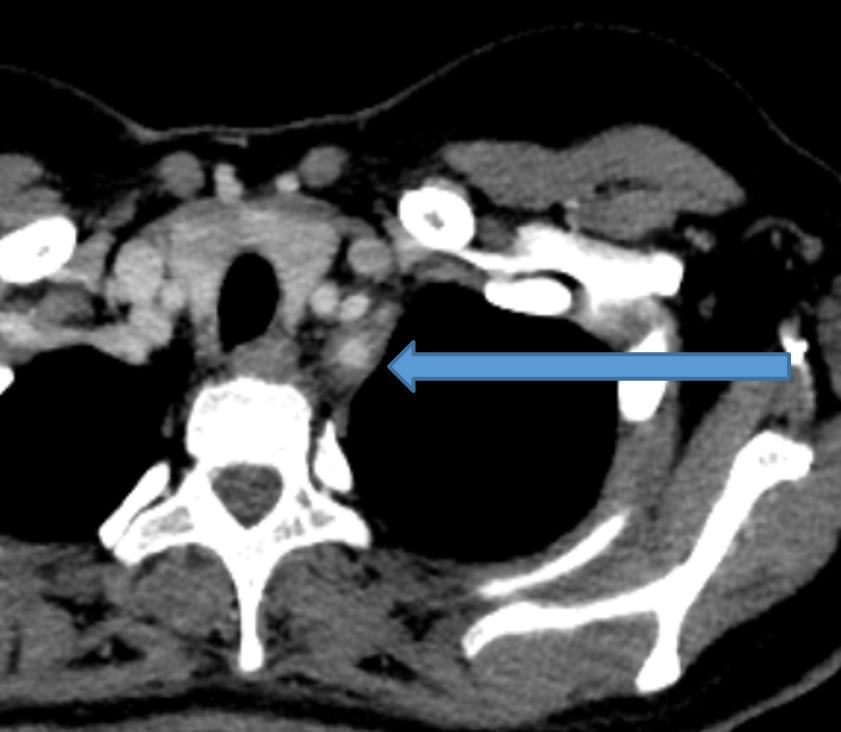
- Concentric wall involving short segment of the proximal portion of left subclavian artery causing mild luminal narrowing (measuring diameter ~ 5 mm).
RADIOLOGICAL DIAGNOSIS:
- Concentric uniform enhancing wall thickening of short segment of the proximal portion of left subclavian artery and left vertebral artery causing mild luminal narrowing.
- Concentric uniform enhancing wall thickening of long segment of the abdominal aorta (from the diaphragmatic hiatus upto the iliac bifurcation). Extension of the wall thickening into the proximal portion of the superior mesenteric artery causing complete luminal occlusion however with distal reformation.
- Mild narrowing at the ostia of the celiac artery and inferior mesenteric artery.
- Concentric uniform enhancing wall thickening of both renal arteries causing luminal stenosis. Horseshoe configuration of the kidneys with atrophic right kidney.
Imaging features are suggestive of aorto-arteritis (Takayasu arteritis) involving predominantly the left subclavian artery, abdominal aorta and its branches.
Discussion:
- Takayasu arteritis is a chronic, idiopathic, inflammatory disease that primarily affects large vessels, such as the aorta and its major branches and the pulmonary and coronary arteries.
- The non-specific inflammation of involved vessels usually leads to concentric wall thickening, fibrosis and thrombus formation. Diseased arteries become stenotic or occluded, undergo vascular remodelling or develop aneurysms.
- Since large-artery biopsies cannot easily be done, imaging examination is essential for providing the diagnosis and differential diagnoses in patients with suspected TA.
According to the vessels involved, the most recently proposed angiographic classification divides TA into 5 types:
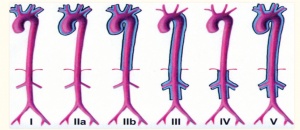
- Type I involves only the branches of the aortic arch.
- Type IIa involves ascending aorta, aortic arch and its branches.
- Type IIb affects ascending aorta, aortic arch and its branches, and thoracic descending aorta.
- Type III involves the descending thoracic aorta, the abdominal aorta and/or the renal arteries. The ascending aorta, the aortic arch and its branches are not affected.
- Type IV involves only the abdominal aorta and/or renal arteries.
- Type V has combined features of Type IIb and IV.
CT Angiography features:
- Concentric mural thickening of the involved arteries
- Calcification in the thickened wall is another important sign of TA
- Calcification is usually transmural
- On pre-contrast CT scanning, the mural thickening is of high attenuation compared with the lumen, while on the post-enhanced CTA images, it exhibits a double ring enhancement pattern, which is typically shown in venous phase.
- Inside ring represents the swollen intima, while the outside ring indicates the active inflammation in the medial and adventitial layers
- Stenosis is the most commonly seen finding associated with mural thickening. Occlusion, ectasis and aneurysm of the vessels can also be seen. Dilatation and aneurysms are usually seen in the ascending and abdominal aorta, respectively.
Treatment
- Treatment is with systemic steroids and judicious use of angioplasty.
- Corticosteroids can be used for initial treatment. Other medical options include methotrexate, cyclophosphamide, and cyclosporine.
- Percutaneous angioplasty and bypass surgery should only be considered when there is no acute inflammation.
- Prognosis tends to be variable, ranging from rapidly progressive disease in some to a quiescent stage in others.
REFERENCE:
- Takayasu arteritis: imaging spectrum at multi-detector CT angiography – F P Zhu et al – BJR Article.
- Takayasu arteritis: evaluation of the thoracic aorta with CT angiography – I Yemada et al – Radiographics.
- Takayasu arteritis: Assessment of coronary arterial abnormalities with 128-section dual source CT angiography of the coronary arteries and aorta – Eun Ju Kang et al – Radiographics.
Dr. VIKHYATH SHETTY
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr. PRIYANKA ROUT
Radiology Resident
Manipal Hospital, Yeshwanthpur, Bengaluru.