
A 40-year gentleman with history of trauma – 3 months back, restricted flexion, posterior knee pain.
Case 1: A 40-year gentleman with a history of trauma – 3 months back, restricted flexion, posterior knee pain.
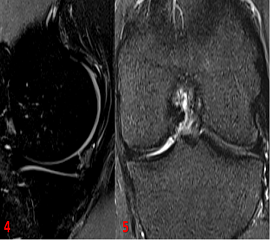
Case 2: A 20-year gentleman with a history of – of injury while playing, now presenting with posterior side left knee pain.
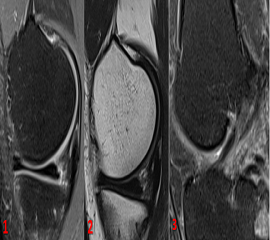
- Sagittal PDFS and T2w images (Fig 1 & 2) demonstrate Ramp lesion (Tear at meniscocapsular attachment posteromedially)
- The sagittal PDFS image (Fig 3) demonstrates anterior cruciate ligament sprain with interstitial tears
- The sagittal PDFS image (Fig 4) demonstrates a tear posteromedially at the meniscocapsular attachment – Ramp lesion.
- The coronal PDF image (Fig) demonstrates a low-grade partial tear involving the anterior cruciate ligament – anteromedial bundle.
DIAGNOSIS:
Case 1: Anterior cruciate ligament sprain with interstitial tears and meniscal Ramp lesion.
Case 2: – Meniscal ramp lesion with low-grade partial tear involving the anterior cruciate ligament.
DISCUSSION:
- Meniscal tears have a significant concomitant prevalence in patients with anterior cruciate ligament (ACL) injury, with reported rates of occurrence as high as 79%.
- Posterior horn of medial meniscus (PHMM) plays an important role in knee instability, particularly regarding to anterior tibial translation.
- Definition of RAMP lesion –“Peripheral vertical longitudinal detachment of the posterior horn of the medial meniscus due to meniscocapsular ligament tears no greater than 2.5 cm in medio-lateral length, leading to meniscocapsular or meniscotibial separation with a concomitant ACL injury”.
- In cases of ACL tear, concomitant ramp lesions may predispose to instability, increased ACL strain and pain, Incidence of ramp lesion increases with chronicity of ACL injury.
- Unstable RAMP lesions – may lead to ACL rupture, ACL graft failure and increased risk of developing osteoarthritis.
- However, due to their location, ramp lesions are easily missed in arthroscopy during standard anterolateral portal and require an additional posteromedial approach. Lack of awareness among reporting radiologists and low preoperative MRI detection also contributes to missed ramp lesions.
- Unrepaired meniscal ramp lesions may cause continued biomechanical deficits despite ACL reconstruction, thereby increasing the risk of graft failure and predisposing to further articular and cartilage damage.
- Pre-operative identification of ramp lesions is therefore essential for optimal surgical management, particularly in cases of concomitant ACL reconstruction.
References:
- Greif DN, Baraga MG, Rizzo MG, Mohile NV, Silva FD, Fox T, Jose J. MRI appearance of the different meniscal ramp lesion types, with clinical and arthroscopic correlation. Skeletal radiology. 2020 May;49(5):677-89.
- Freire G, Jesus M, Afonso PD. Meniscal “ramp” lesions: how can we detect them on MRI? European Congress of Radiology-ESSR 2019.
Dr. Vivek J, MD
Senior resident & Cross Section fellow
MHRG
Dr. Dayananda Sagar G, MD
Consultant radiologist
MHRG