

9 year old girl presenting with pain in right arm. Past history of multiple hospital admissions for bone pain since the age of 5
A 9-year-old girl presented with pain in her right arm. Past history of multiple hospital admissions for bone pain since the age of 5.
On admission
MRI on prior admission 7 months back
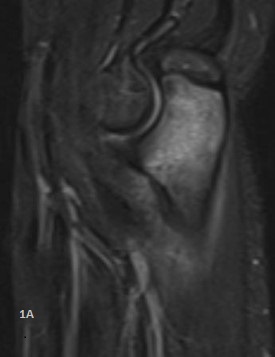

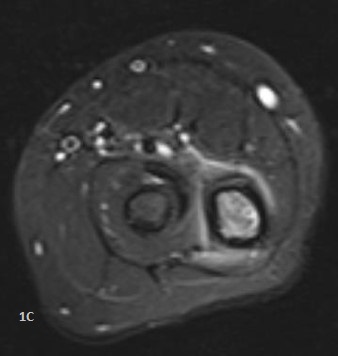

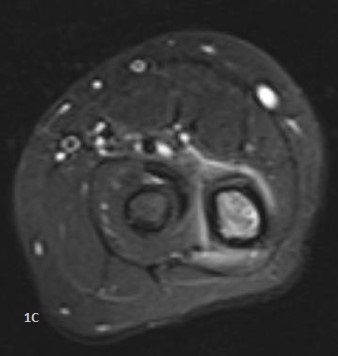
- Sagittal STIR (Fig:1A), T1 (Fig:1B) and axial STIR (Fig:1C) images demonstrates marrow edema in proximal Ulnar metaphysis with mild surrounding periosteal reaction and soft tissue edema.
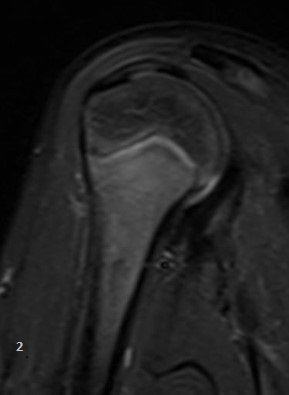
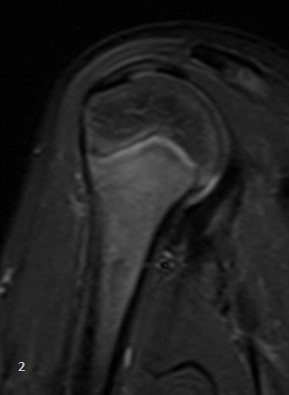
- Oblique STIR (Fig:2) image of upper Humerus demonstrates marrow edema in proximal Humeral metaphysis extending into diaphysis.
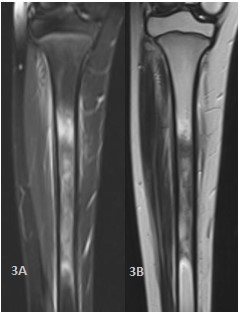
- Coronal STIR (Fig:3A), T1 (Fig:3B) and axial STIR (Fig:3C) demonstrates marrow edema in mid-shaft of Tibia with mild surrounding periosteal reaction.
- Axial STIR (Fig:4) image of ankle demonstrates marrow edema in Calcaneus.




Diagnosis:
Chronic Recurrent Multifocal Osteomyelitis (CRMO)
Discussion:
- Chronic recurrent multifocal osteomyelitis (CRMO) / Chronic non-bacterial osteomyelitis (CNO) is an autoinflammtory skeletal disorder, primarily affecting children in 7-14 years age group with female preponderance.
- Typical clinical features include waxing and waning bone pains, swelling or limited range of movement at one site, changing to other sites over a period of time.
- Biopsy may be nonspecific with features of inflammation. Cultures for micro organisms are typically sterile. Inflammatory markers may be mildly elevated during active phase.
Common sites of involvement: Metaphysis of long bones of lower limbs; frequently spine, pelvis and feet may be involved.
- Involvement of medial clavicle and mandible is less common but when present, CRMO is a strong possibility.
Imaging
- Conventional radiography: Small lytic lesions adjacent to growth plates, which may enlarge and progressively become sclerotic.
- Role of CT and FDG/ PET scans is limited due to radiation dose and non specificity.
- MRI is most sensitive- active disease demonstrating multiple foci of marrow edema on STIR/ PDFS images, often in metaphysis.
MRI also demonstrates periostitis, soft tissue inflammation, synovitis and transphyseal extension.
- If left untreated sclerosis, collapse and growth deformities can occur.
- Role of whole body STIR is evolving, with this single sequence useful for demonstrating multiple hidden areas of involvement which can be further characterized.
-
Differential diagnosis
- Bacterial osteomyelitis: Significant adjacent inflammatory changes, abscess formation, sinus tracts, or deep venous thrombosis which are rare in CRMO.
- Focal peripheral edema (FOPE): may be related to microtrauma, adolescents 12- 16 years, solitary focal edema on STIR centered at the physis with adjacent extensions and resolving spontaneously. Typically seen around the knee.
- High turnover marrow: Multiple foci of increased STIR signal in multiple bones of hind feet in children younger than 15 years; however it is less focal than CRMO.
-
Finally, it must be remembered that CRMO is a diagnosis of exclusion; a proper history, follow up and awareness of this condition helps in arriving at a correct diagnosis.
Dr. Sushant Mittal
Senior resident &Cross sectional fellow
CARG
Dr Dayanand Sagar G
Consultant Radiologist
CARG