
A 59-year old male with pain in upper abdomen on right side since 1 week, nausea and vomiting episodes after having food since 2 days and constipation since 2 days. He also complained of increased frequency of micturition
A 59-year-old male with pain in the upper abdomen on the right side for 1 week, nausea and vomiting episodes after having food for 2 days, and constipation for 2 days. He also complained of increased frequency of micturition

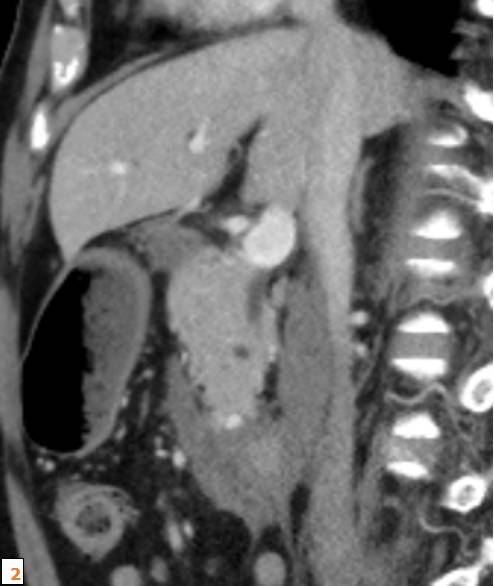

- There is compression of the celiac axis just distal to origin with a post-stenotic dilatation (Fig 1a).
- There is a tiny speck of hyperdensity along the inferior pancreatic arcade – measuring ~ 4mm (Fig 2a).
- Moderate circumferential hyperdense asymmetrical intra mural wall thickening is seen in the D2 and D3 segments of duodenum for a length of ~8 cm. Moderate amount of fat stranding is seen surrounding this segment of duodenum and pancreaticoduodenal groove (Fig 3a).
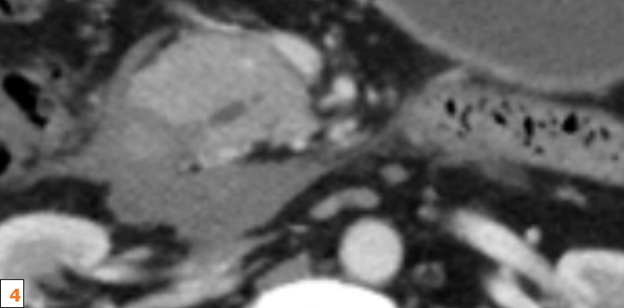
- Mild dilatation of the main pancreatic duct (maximum width = 4.2 mm), likely secondary to ampullary edema (Fig 4a).
Diagnosis:
Retroperitoneal periduodenal hematoma caused by leaking Arc of Buhler Aneurysm / inferior pancreaticoduodenal arcade aneurysm secondary to Median arcuate ligament syndrome
Discussion:
- The Arc of Buhler (AOB) is a persistent embryonic ventral anastomosis between the Celiac trunk and the Superior mesenteric artery. It arises from failure of this regression of this persistent ventral communication between the SMA and the celiac trunk or one of its branches and provides a collateral pathway between these vessels.
- The causes of abdominal visceral artery aneurysms include stenosis at the origin of the celiac artery, arteriosclerosis, trauma, infection, pancreatitis, and tumor.
- In Median arcuate ligament syndrome (MALS), the median arcuate ligament compresses and constricts the celiac artery. Consequent intraluminal pressure differences between the superior mesenteric and celiac arteries increases compensatory blood flow in the Arc of Buhler (AOB), which opens up as a direct collateral anastomotic artery between these two territories. The resultant increase in arterial blood pressure weakens the arterial wall and an aneurysm develops.
- Symptoms like hematemesis or hemorrhagic stool and acute abdomen may develop if it ruptures into gastrointestinal tract and abdominal cavity, respectively. If the rupture occurs into the retroperitoneal space, the affected individual usually has no symptoms other than anemia.
- Although the management of this aneurysm is unclear, with advances in interventional radiology, coil embolization is the first choice of treatment.
- Importantly, embolization of this aneurysm may result in a significantly greater blood flow at other vessels such as a pancreaticoduodenal artery resulting in recurrence of the aneurysm. Hence, careful and long-term follow-up is necessary
DIFFERENTIAL DIAGNOSIS:
Closely related differential diagnosis to the AOB aneurysm is the pancreaticoduodenal artery arcade (PDAA) aneurysm.
REFERENCES:
- Biswas S, Gogna S. Arc of Buhler Pseudoaneurysm Causing Fatal Retroperitoneal Hemorrhage; A Rare Case Report and Discussion of Relevant Literature. Bulletin of Emergency & Trauma. 2019 Apr;7(2):183.
- Abe K, Iijima M, Tominaga K, Masuyama S, Izawa N, Majima Y, Irisawa A. Retroperitoneal Hematoma: Rupture of Aneurysm in the Arc of Bühler Caused by Median Arcuate Ligament Syndrome. Clinical Medicine Insights: Case Reports. 2019 Feb;12:1179547619828716.
Dr. Rajesh Helavar
MD Radiology, PDCC Gastro Radiology
Consultant Diagnostic and Interventional Radiology
Manipal Hospitals Radiology Group.
Dr. Vivek Jirankali
Senior Resident and Cross-sectional fellow
Manipal Hospitals Radiology Group.