
46 year old female, history of fall and injury to left thumb 5 months back presenting with persistent pain and weakness of grip
46-year-old female, history of fall and injury to left thumb 5 months back presenting with persistent pain and weakness of grip.


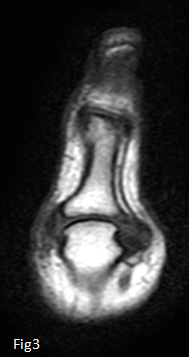
Coronal PDFS images (Fig 1 and Fig 2) of metacarpophalangeal joint of thumb demonstrates complete tear of ulnar collateral ligament of thumb with retraction of proximal fibers. Note the abnormal horizontal orientation of torn proximal ligament fibers. Fig 2 demonstrates an intact radial collateral ligament. Marrow edema and small osteophyte noted at the base of proximal phalanx on ulnar side
Coronal T1 images demonstrate scarred and clumped up capsule & ligament fibers on ulnar side of metacarpophalangeal joint of thumb.
DIAGNOSIS:
Complete tear of ulnar collateral ligament (UCL) of thumb with retraction – Stener lesion.
DISCUSSION:
RELEVANT ANATOMY:
- UCL and RCL are primary static stabilizers of MCP joint of thumb.
- UCL comprises of proper and accessory bands (Not separable on MRI)
- Proper UCL extends obliquely from dorsal ulnar aspect of metacarpal head to volar portion of base of proximal phalanx.
- Adductor aponeurosis drapes over and lies superficial to UCL
ULNAR COLLATERAL LIGAMENT INJURIES OF THUMB
- UCL injuries are among common injuries of hand resulting from forced valgus stress at MCP Joint.
- X-ray may demonstrate an avulsion fracture at the base of proximal phalanx on ulnar aspect. Absent or minimally displaced fracture does not exclude an underlying ligament injury
MRI features of UCL tears:
- Abnormality in orientation, signal and contour of ligament
- Complete tears are identified by hyperintense signal fully traversing the ligament or at its bony attachment on fluid sensitive sequences
- Focal attenuation of ligament with hyperintense signal partially traversing the ligament indicates partial tear
- Stener lesion refers to complete tear of UCL from distal attachment with retraction proximal to proximal margin of adductor aponeurosis.
- Sterner lesions are better appreciated on coronal images – torn ligament remains attached at metacarpal head with an abnormal clumped up contour.
- Abnormal orientation of ligament projecting ulnarly (Normal orientation is vertical towards proximal phalanx).
- Low signal proximal margin of adductor aponeurosis may be seen distal to and abutting the torn ligament.
- Tear of UCL without retraction/displacement is not Stener lesion.
Because the torn end of ligament is blocked from reapproximating the site of insertion, spontaneous healing is not achieved resulting in instability. Surgical correction is indicted in repair of Stener lesion.
Dr Dayanand Sagar G, MD
Consultant Radiologist MHRG
Dr Shashwat Priyadarshi, DNB
Cross sectional imaging fellow MHRG