

31 years male history of RTA, presenting with severe left leg pain
31y, Male History of RTA, presenting with severe left leg pain
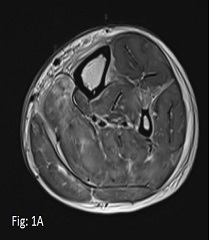
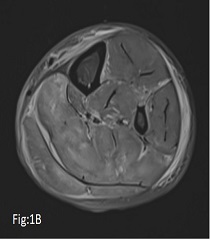


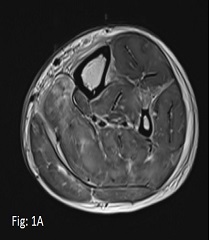
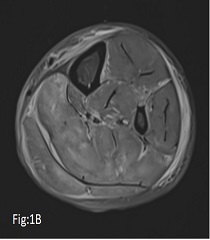
- Fig:1A (Axial T2), Fig:1B (Axial STIR) & Fig:1C (Coronal STIR) demonstrates extensive intramuscular edema involving muscles in all the compartments of leg with perifascial fluid and subcutaneous soft tissue edema. Note is made of fracture proximal Tibia.
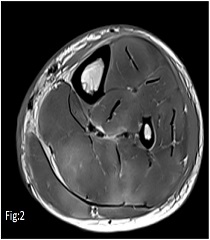
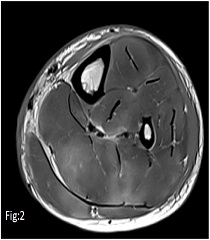
- Fig:2 (Axial T1): Poorly circumscribed intramuscular T1 hyper intense areas suggestive of intramuscular hemorrhage.
- Fig:3 (Sagittal STIR): Zoomed image demonstrating on of the focal muscle herniation.


COMPARTMENT SYNDROME
- Elevated pressure within a relative non-compliant anatomical compartment resulting in ischemia and sequelae.
- Acute compartment syndrome is a surgical emergency, if not intervened early, may lead to:
- Acute compartment syndrome Neuromuscular injury, myonecrosis and rhabdomyolysis.
- Chronic compartment syndrome Fibrosis and scarring: “Volkmann ischemic contracture”
ETIOLOGY
- Acute: Fractures.
- Chronic: Exercise, overuse, accessory muscles, SOL, infection.
CLINICAL FEATURES: 6 “P”s
-
- Pain
- Pallor
- Paraesthesia
- Paresis
- Pulselessness
- Poikilothermia
“ Distal pulse may be normal in early acute compartment syndrome”
MR IMAGING FEATURES
- Increased T2/STIR signal: Muscle edema (acute & chronic).
- Increased T1 signal: Hemorrhage (acute), fatty infiltration (chronic).
- Decreased T1 signal: Fibrosis, calcification (chronic).
- Increased muscle volume (acute) / decreased muscle volume (chronic).
- Bulging fascial outline (acute).
- Muscle herniations (acute).
- Fascial thickening (chronic).
CHRONIC EXERTIONAL COMPARTMENT SYNDROME
- Common in athletes, type of over-use injury
- Pain or sense of pressure in limbs typically after exertion.
- Increase in muscle bulk and edema post exertion.
- May co-exist with underlying bone stress features like periosteal edema or fatigue fractures.
DIFFERENTIAL DIAGNOSIS
- Delayed onset muscle soreness (DOMS)
- Muscle strain
- Deep venous thrombosis.
- Cellulitis and lymphedema.
Dr. Sushant Mittal
Senior resident & Cross sectional fellow
CARG
Dr. Dayanand Sagar G
Consultant Radiologist
CARG