
A 38 year old patient presenting with headache and dizziness since 15 days. Past history of surgically treated squamous cell carcinoma right buccal mucosa.
A 38 year old patient presenting with headache and dizziness since 15 days. Past history of surgically treated squamous cell carcinoma right buccal mucosa.
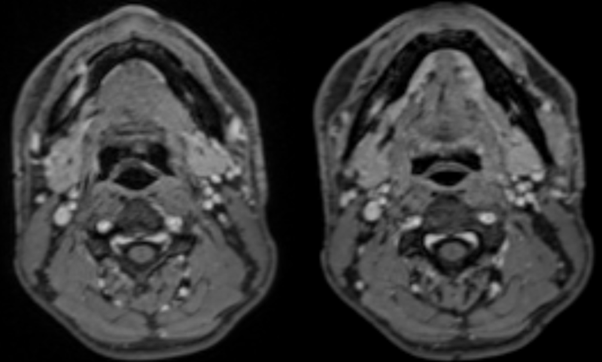
- Axial contrast enhanced T1 fat-suppressed sequences at the level of the mandibular ramus demonstrate nodular focal enhancement at the right mental foramen. This is contiguous with abnormal thickening and enhancement in the right mandibular canal which contains the inferior alveolar nerve. Note normal enhancement of the left inferior alveolar nerve.
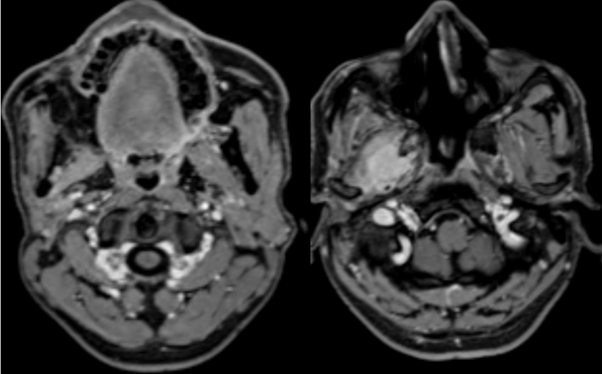
- Axial contrast-enhanced T1 fat-suppressed sequences at the level of the mandibular ramus and infratemporal fossa demonstrate abnormal enhancement and thickening in the right mandibular foramen as compared to the contralateral side. Bulky mass like enhancement is also noted in the right infratemporal fossa involving the pterygoid musculature and the body of pterygoid which demonstrates abnormal marrow enhancement.
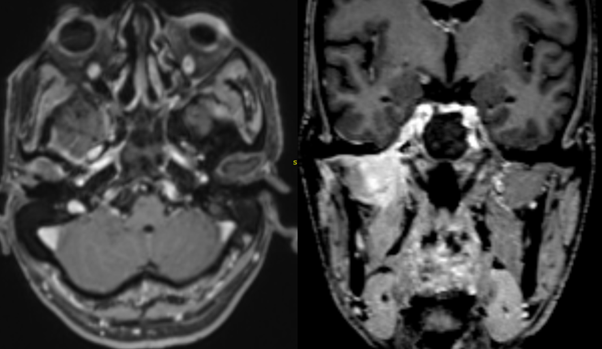
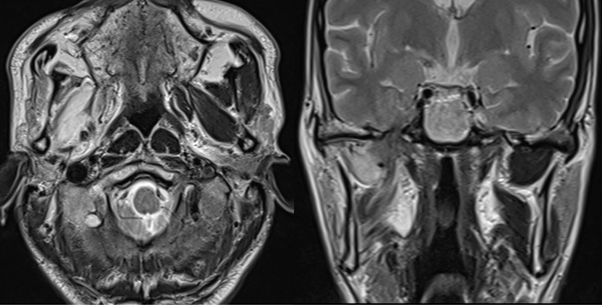
- Axial and coronal contrast-enhanced T1 fat-suppressed sequences demonstrate marked widening of the right foramen ovale with abnormal enhancement of the right mandibular nerve extending intracranially to involve the right cavernous sinus.
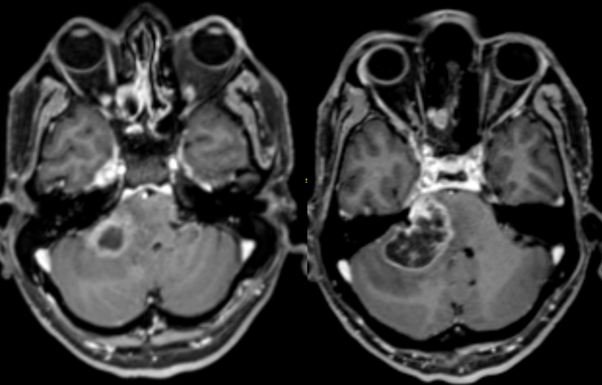
- There is further retrograde involvement with abnormal mass like enhancement in the Meckel’s cave, extending posteriorly into the right cerebello-pontine angle and brainstem.
- Axial and coronal T2-weighted sequences demonstrate secondary denervation oedema in the right lateral and medial pterygoid and masseter muscles.
Perineural spread of squamous cell carcinoma along right inferior alveolar nerve to the right infratemporal fossa, right mandibular nerve, cavernous sinus, Meckel’s cave and along the right trigeminal nerve to the right cerebellopontine angle and brainstem.
Discussion:
Head and neck malignancies showing propensity for perineural spread include:
- Squamous cell carcinoma
- Adenoid cystic carcinoma
- Malignant desmoplastic melanoma
- Basal cell and adenocarcinoma
Modalities for diagnosis:
- CT has low sensitivity. Bony foramina better evaluated.
- MRI is the preferred modality due to superior soft tissue contrast.
Indicators of perineural spread:
- Effacement of perineural, foraminal and/or juxtaforminal fat
- Asymmetric nerve or foraminal enlargement
- Asymmetric, irregular or nodular nerve enhancement
- Secondary features of denervation injury including acute edema and chronic atrophy.
Key anatomic landmarks:
- V1: Supraorbital foramen.
- V2: Infraorbital foramen, pterygopalatine fossa, vidian canal, foramen rotundum, greater and lesser palatine foramen.
- V3: Mental foramen, mandibular canal, mandibular foramen, foramen ovale
- Facial nerve: Mastoid segment and stylomastoid foramen
- Hypoglossal nerve: Hypoglossal canal
Potential sources of pitfalls:
- Recurrence of disease after some time of treatment where a primary lesion may not always be appreciated (detailed history should be obtained)
- Normal enhancement of foramen (comparison with opposite normal side is important)
- Evidence of skip lesion (full course of nerve should be evaluated closely).
Perineural spread of malignancy is a potential and important route of spread of head and neck malignancies; its presence indicate a poor prognosis. A checklist approach and thorough inspection of potential sites on contrast enhanced fat-suppressed images should be routinely undertaken.
The presence of focal neurological deficits and cranial nerve palsies in patients with head and neck malignancies should prompt a detailed search to exclude perineal spread of malignancy.
References:
- Perineural Tumor Spread in Head and Neck Malignancies, Seminars in Roentgenology, Volume 54, Issue 3, 2019, Mohit Agarwal, Pattana Wangaryattawanich, Tanya J. Rath.
- Perineural spread in head and neck malignancies, Radiation Medicine volume 24, pages1–8(2006). Ojiri, H.
- Perineural spread of malignant head and neck tumors: review of the literature and analysis of cases treated at a teaching hospital. Mauro César Silveira Moreira, Antonio Carlos dos Santos, Murilo Bicudo Cintra. Radiol Bras. 2017 Sep-Oct; 50(5): 323–327
Dr. Sushant Mittal,
MD, Cross-sectional Fellow,
Manipal Hospitals Radiology Group.
Dr. Anita Nagadi,
MD, MRCPCH, FRCR, CCT (UK)
Lead Head & Neck, Oncology
Senior Consultant Radiologist
Manipal Hospitals Radiology Group.