
46 year old gentleman presented with complaints of left sided lower abdominal pain, mild swelling and heaviness
46 year old gentleman presented with complaints of left sided lower abdominal pain, mild swelling and heaviness




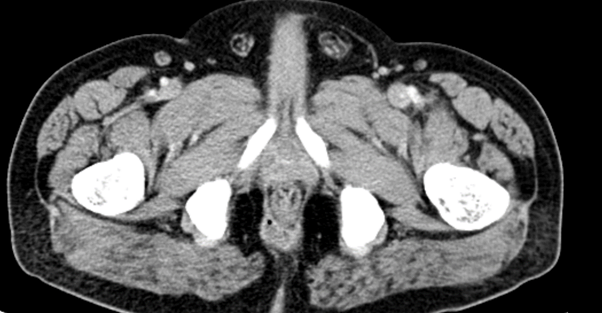
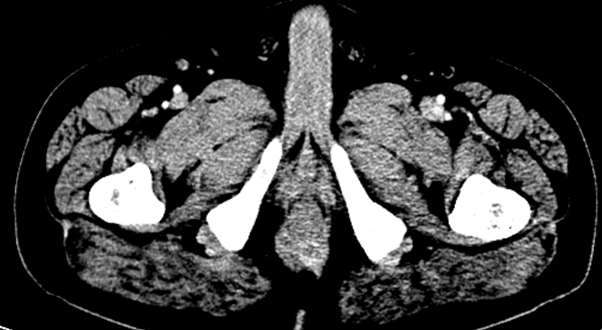
- A trans sphincteric peripherally enhancing collection (Figure A) with supra levator extension (Figure B) is seen on the right side.
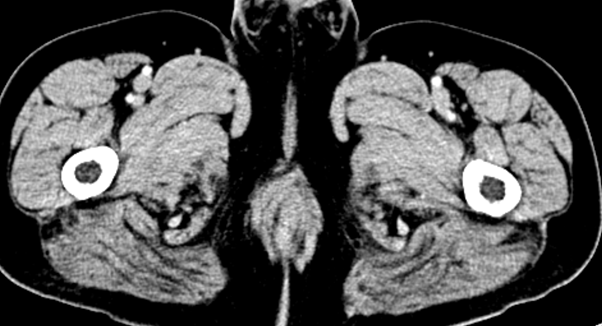
- A peripherally enhancing horse shoe shaped abscess (Figure C) with a few air foci (Figure D) within is seen in the perianal region at 5 to 8 o clock position extending to the right ischioanal fossa. Mild enhancing thickening of the anal canal and the external sphincter (Figure D)
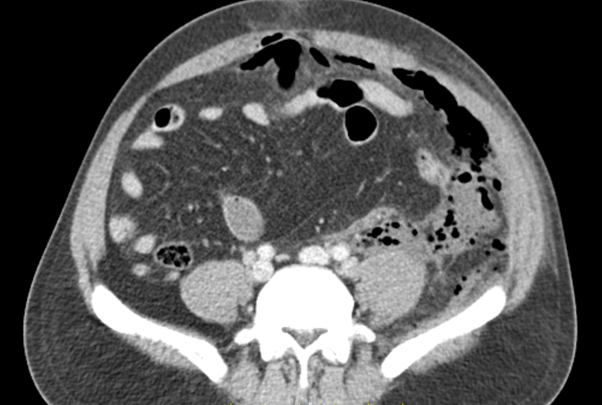
- Superior extension of collection to the right pelvic sidewall abutting the right obturator muscles, pro-peritoneal space anterior to the urinary bladder (pre vesical space of Retzius) demonstrating hyperdense fluid with mottled air foci (Figure E)
- Extension to beneath the anterior and left lateral abdominal wall, posterior to the left latero-conal and posterior renal fascia into the posterior pararenal space, along the left psoas with pneumo retro peritoneum (Figure F,G,H)
- Mild left perinephric fluid and a few air foci in the left perinephric space with normal bulk and enhancement of the left kidney (Figure I)

Diagnosis:
Widespread Pro-peritoneal and Retroperitoneal Abscess secondary to Complex Trans Sphincteric Fistula in-ano with Supra-levator Extension (Grade 5)
Discussion:
- Suppurative disease of the rectum and peri-rectum is common ailment and the suppuration is usually located below the level of the pubo-rectalis muscle.
- If not diagnosed and adequately treated at this stage, more than 90 % of these collections will rupture.
- As the pubo-rectalis sling exerts a strong pressure on the posterior rectal wall at the anorectal ring preventing supra levator extension of abscess, these collections will usually rupture through the longitudinal muscle and extend trans-sphincterically into one of the infra levator anorectal spaces.
- But rarely, a low intermuscular abscess may extend above the level of the pubo-rectalis muscle to form a high intermuscular abscess, which may rupture into one of the supra levator spaces.
- Supra levator abscesses can spread to the pre vesical space, as there is a direct communication from para rectal space to the vesicle extra peritoneal space without a separating fascial layer due to the umbilicovesical fascia ending at the reflection of the vesical peritoneum.
- From the pre vesical space, the infection can spread through the anterior space of Retzius anteriorly, as well as into other pelvic compartments, and to the retro peritoneum posteriorly, through direct spread.
- Retroperitoneal region reacts to bacterial contamination to a lesser extent compared to the intra peritoneal region and tend to follow a more indolent and asymptomatic course leading to delayed diagnosis and treatment. This may lead to higher rate of sepsis and increase the mortality risk.
- Clinicians can only partially evaluate the retro-peritoneum during the physical examination, and laboratory investigations provide limited information. Therefore, radiological investigations, especially computed tomography can play a key role in the diagnosis.

Schematic diagram demonstrating the retroperitoneal spaces
Reference: clinicalradiologyonline.net, https://europepmc.org/article/pmc/6698495


Contrast-enhanced CT scan at the level of right renal hilum (a, b) and iliac crest in a case of duodenal perforation (c) shows the retroperitoneal and interfascial planes.
- Anterior pararenal space (APS) is limited by posterior parietal peritoneum and anterior renal fascia, with midline continuity; posterior pararenal space (PPS) between posterior renal fascia and transversalis layer of endoabdominal fascia; perirenal space (PS) between anterior and posterior renal fascias. Renal and lateroconal fasciae are laminated, defining potential spaces: the retro mesenteric (RMP), the retrorenal (RRP) and lateroconal planes (LP) that all communicate at fascial trifurcation.
- Axial image focused on fascial trifurcation. Ectopic gas is seen extending through the retro mesenteric plane (RMP), retrorenal plane (RRP) and lateroconal plane (LP), and meeting at the fascial trifurcation (red star). Posterior pararenal space (PPS) anteriorly continues as a fat stripe in the properitoneal space (PP).
- Inferior extension of the interfascial plane, delineated by ectopic gas/air. The retro mesenteric and the retrorenal planes approximate one another as the fat cone of perirenal fat diminishes inferiorly, resulting in the combined interfascial plane (CIP); it continues in the pelvis along the anterolateral margins of the psoas muscle contiguous with the pelvic retroperitoneal peri vesical and presacral spaces
- Contrast-enhanced CT scan at level of acetabular dome shows endopelvic fascia and extra peritoneal pelvic spaces.
Conclusion:
This case highlights:
1. The complex anatomic compartments and potential spaces that allow a benign and common perirectal abscess to extend into the abdomen.
2. The importance of looking closely at rectum and anal canal for a Fistula in ano as source of infection.
Imaging differentials:
- Perforated retroperitoneal hollow viscus :
- duodenum
- peptic ulcer disease
- blunt or penetrating abdominal trauma
- iatrogenic
- ascending/descending colon
- colorectal carcinoma (CRC)
- diverticulitis
- endoscopy +/- biopsy
- ischemic colitis
- rectum
- surgery
- foreign body insertion
- endoscopy
- trauma
- duodenum
- Fournier gangrene
- Emphysematous pyelonephritis with retroperitoneal abscess
REFERENCES/ FURTHER READING:
- https://www.sciencedirect.com/science/article/pii/S221156841400206X
- https://hsc.ghs.org/wp-content/uploads/2016/05/GHS-Proc-Complex-Space-Retzius-Abscess.pdf
- https://www.jpgmonline.com/article.asp?issn=0022-3859;year=1987;volume=33;issue=2;spage=97;epage=8;aulast=Zaveri
- https://www.sciencedirect.com/science/article/pii/S2049080117302030
- https://radiopaedia.org/articles/pneumoretroperitoneum
- https://link.springer.com/article/10.1007/s13244-013-0278-0#citeas
Dr. Rosmi Hassan
PG , Manipal Hospitals Radiology Group.
Dr. Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Manipal Hospitals Radiology Group.
Dr. Vineetha Raghu
MD, DNB
Consultant Radiologist
Manipal Hospitals Radiology Group.