
Incidentally noticed abdominal lump; no constipation, no urinary retention or any other complaints. Growth and development - normal
- Incidentally noticed abdominal lump
- No constipation, no urinary retention or any other complaints
- Growth and Development - normal
Examination:
- Ill defined ballotable mass.
- No organomegaly or lymphadenopathy.
FINDINGS:
- CT CHEST, ABDOMEN PELVIS WITH IV CONTRAST



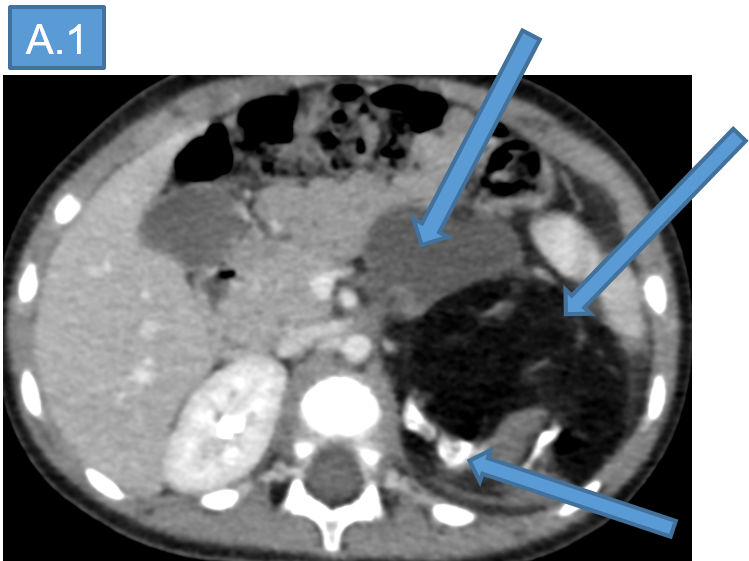
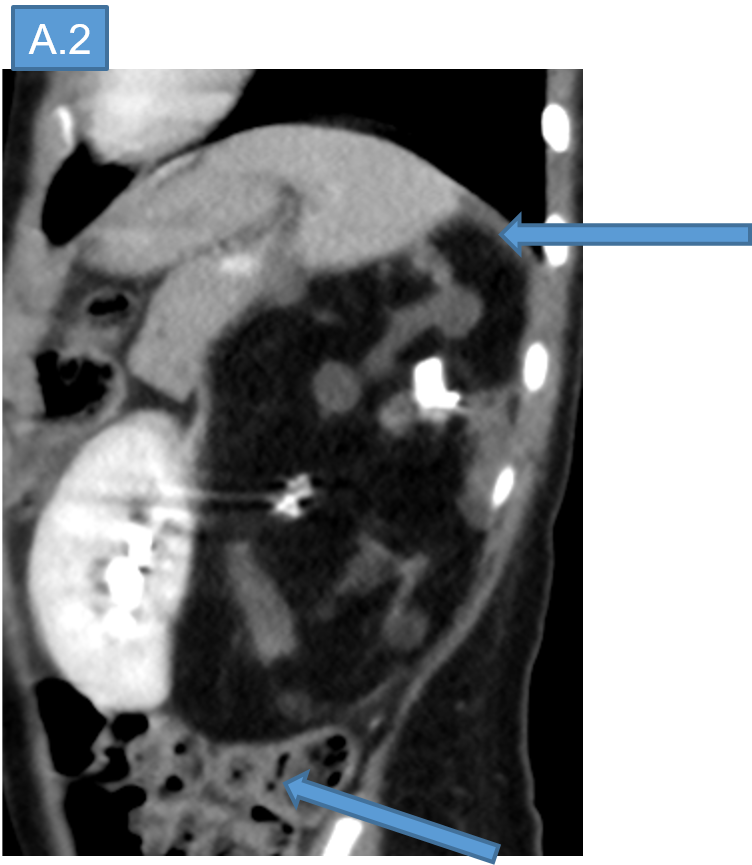
- A.
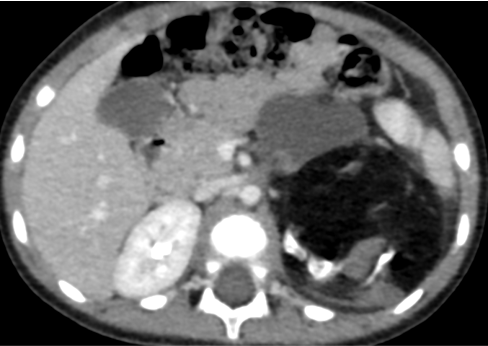
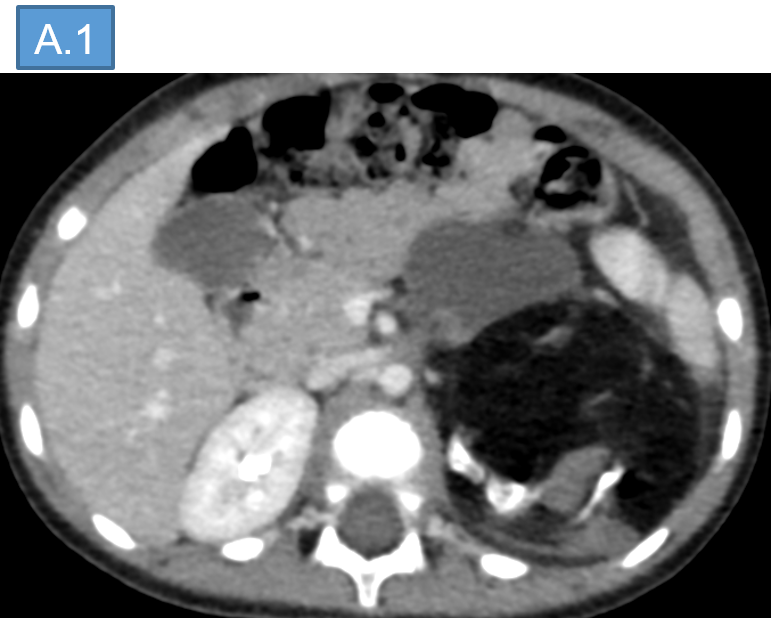
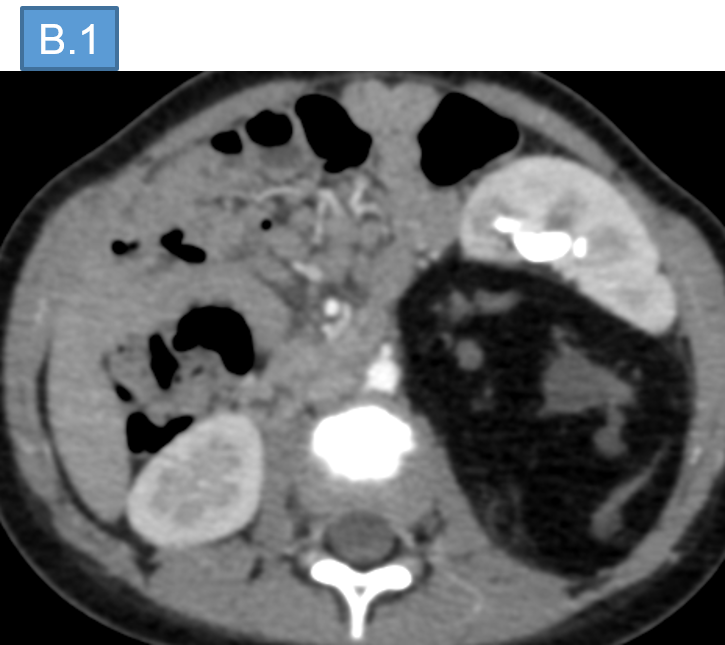
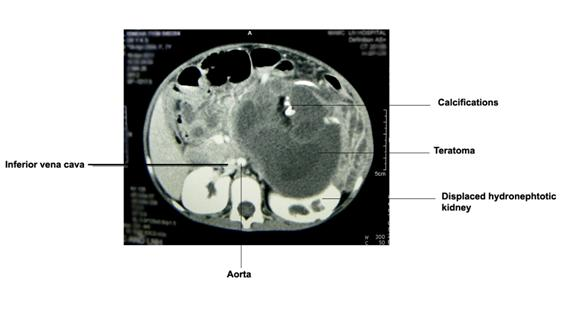
- The lesion is composed of large fatty attenuation components, few foci of ossification and multiple cystic components.
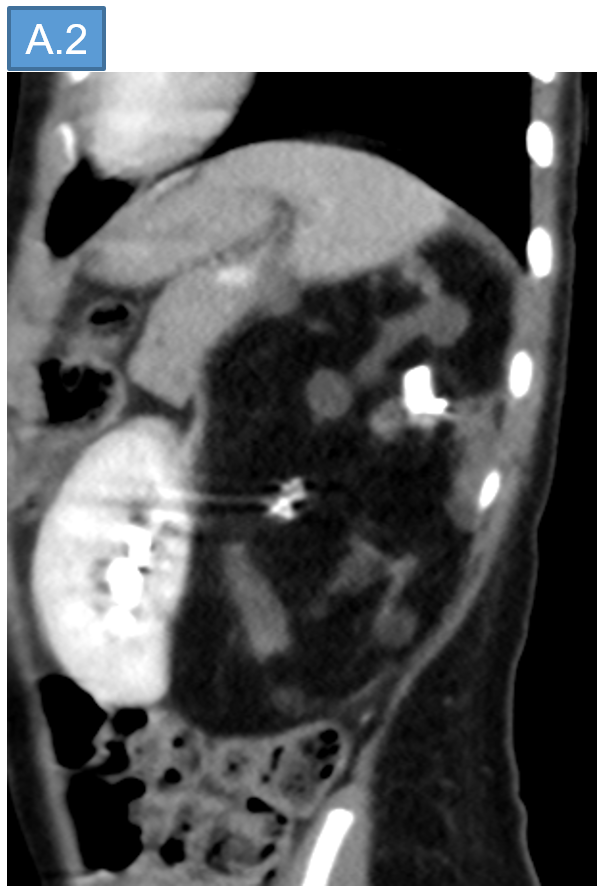
- Superiorly the lesion extends upto the left subdiaphragmatic space and inferiorly the lesion is displacing adjacent bowel loops.
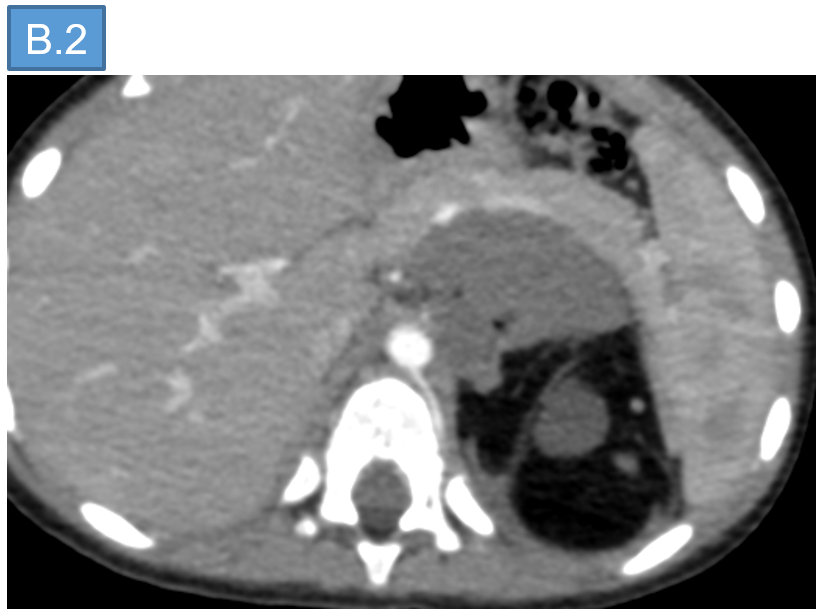
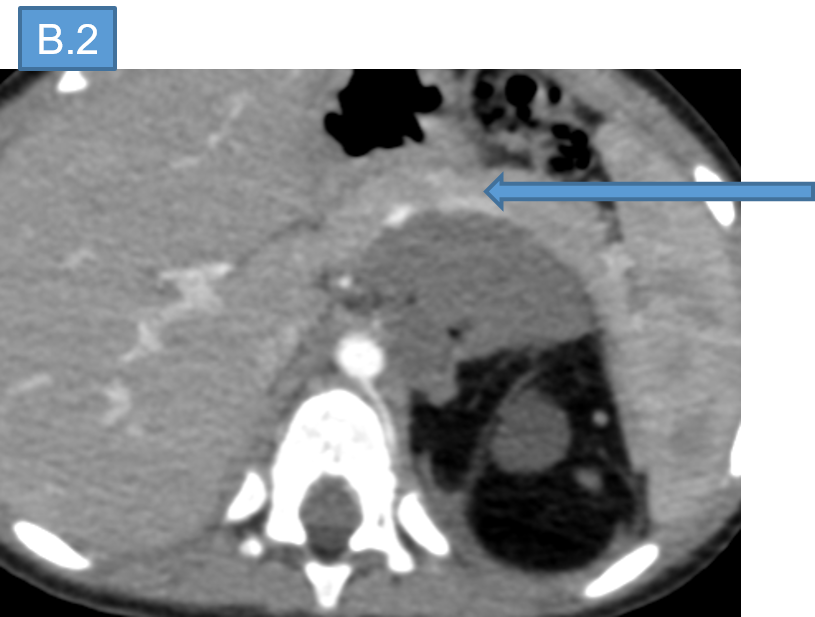
- B. Anteriorly the lesion abuts and displaces the left kidney with secondary compression on the renal pelvis, abuts the body and tail of pancreas.
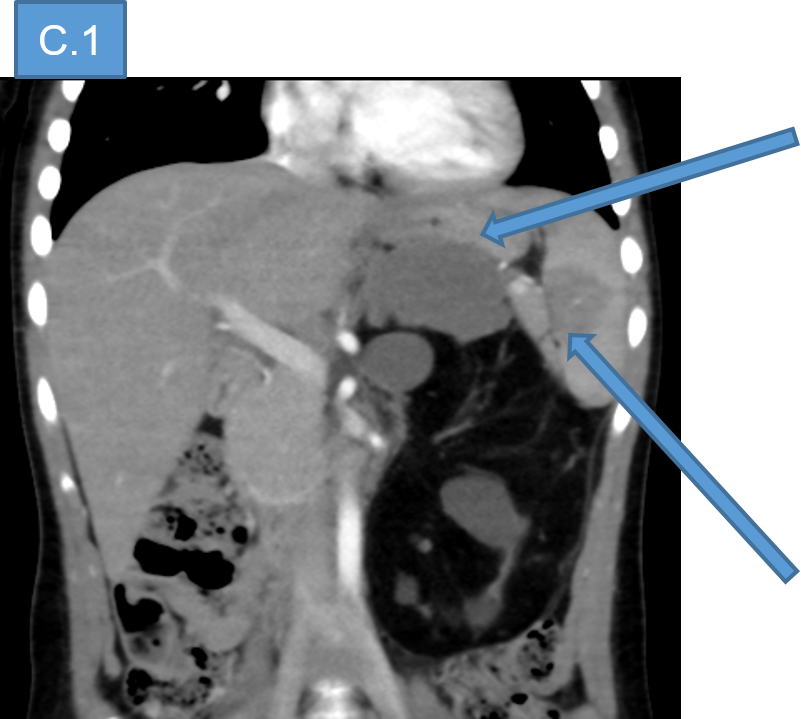
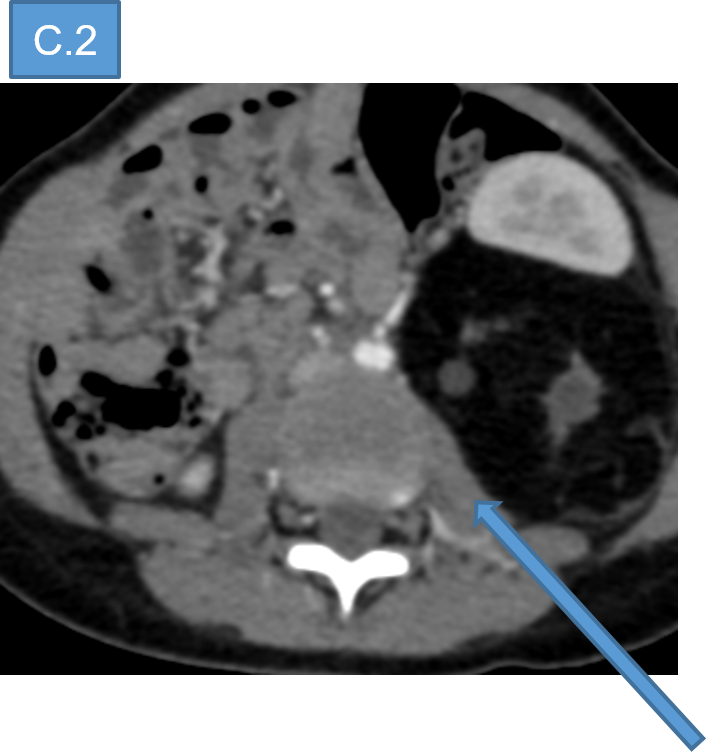
- C.
- Superiorly, the lesion abuts fundus of stomach, and the spleen.
- Posteriorly the lesion is abuts the left psoas muscle.
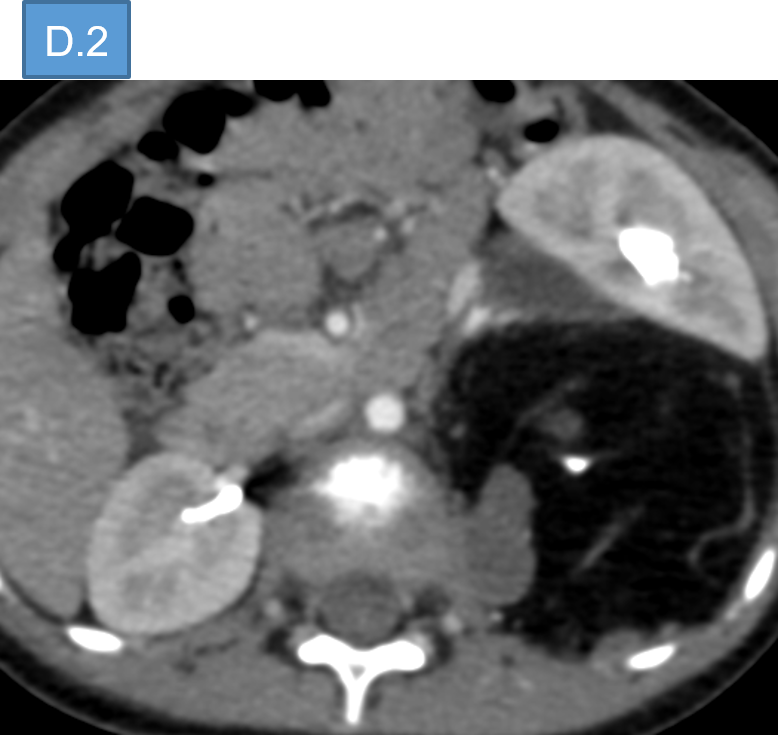
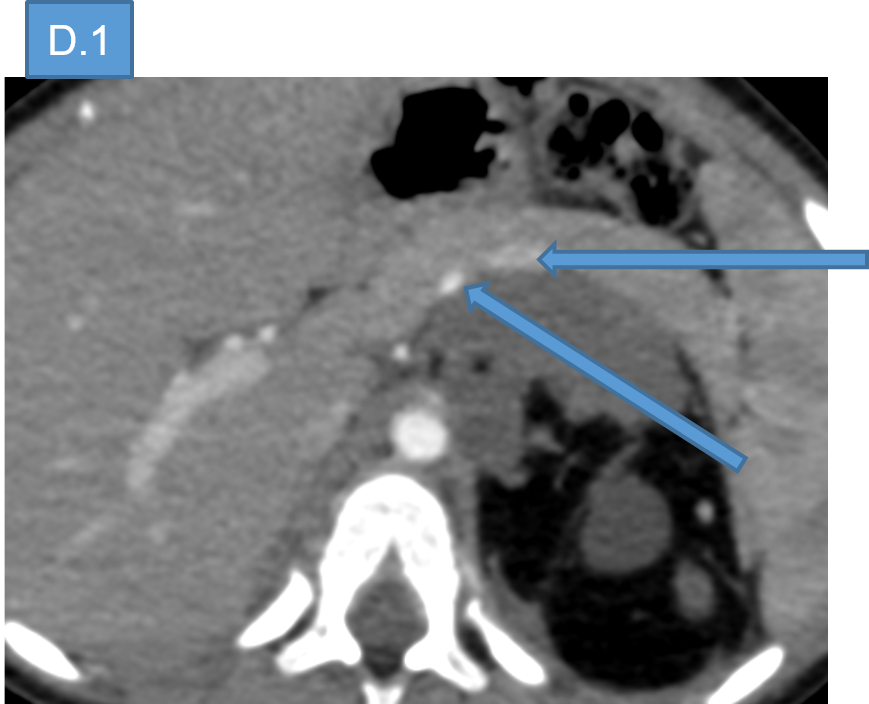
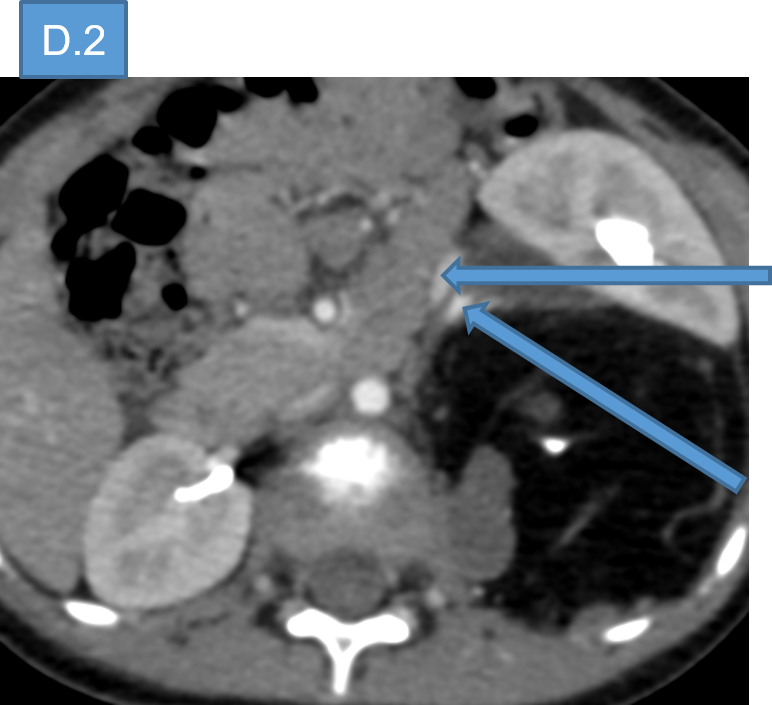
- D. The splenic artery and vein, left renal vein and artery are coursing along the anterior margin of the lesion.

DIAGNOSIS:
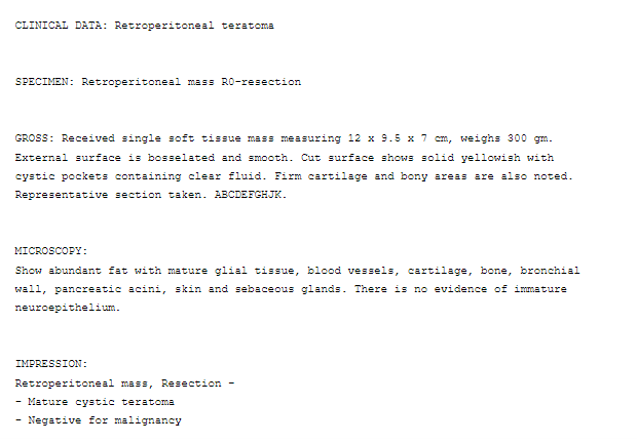
- Non secretory Germ cell tumor – Teratoma.
DISCUSSION:
- Germ cell tumors are broadly classified as gonadal or extra gonadal depending on their site of origin.
- The extra-gonadal distribution of teratomas in order of decreasing frequency is as: the anterior mediastinum, the retroperitoneal space, the presacral and coccygeal areas, pineal, and other intracranial sites, the neck and abdominal viscera.
- Teratoma consisting of tissue derived from embryonic ectoderm, mesoderm and endoderm are the most common extragonadal germ cell tumors in children.
- In general, the prognosis of pediatric EGCTs worsens with increasing age.
- Pediatric EGCTs can be further classified into
- presenting during the congenital/neonatal period (birth to 6 months),
- during childhood (7 months–12 years)
- after 12 years,
- with the youngest age group having the most favorable prognosis and lowest recurrence rate.
- Usually, retroperitoneal teratomas are asymptomatic.
- Symptoms - back or abdominal pain, GI symptoms secondary to compression of adjacent structures.
- Signs - palpable abdominal mass, tenderness, and distension.
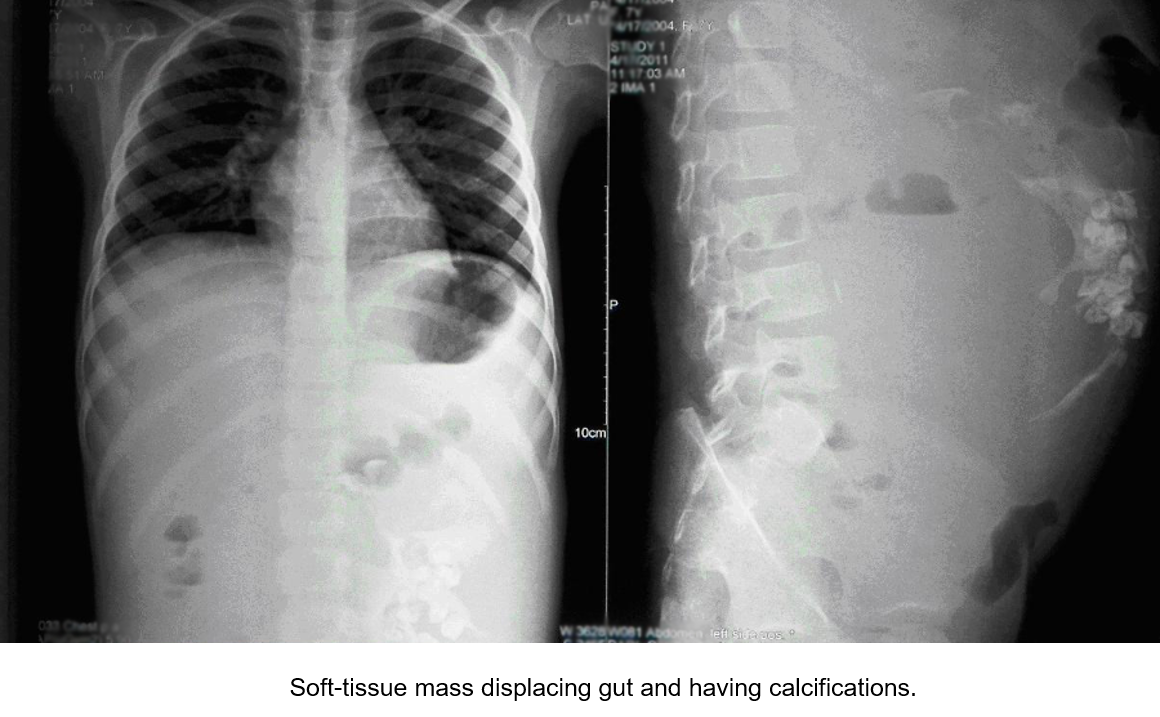
PLAIN RADIOGRAPH:
- soft tissue mass with calcification
- opacity or a radiolucent mass that displaces the digestive spaces
USG:
- acoustic shadow and occasionally fat-fluid levels.
- can be cystic or completely solid in appearance.

CT:
- Complex mass containing well-circumscribed fluid component, adipose tissue, and calcification.
- Presence of fat-fluid levels in peritoneum is reliable sign of intraperitoneal rupture.
MRI:
- Demonstrates invasion of the adjacent organs and delineating cyst contents.
Differential diagnosis of retroperitoneal teratomas can be:
- Renal cyst
- Lymphadenopathy
- Adrenal tumors
- Retroperitoneal fibromas
- Sarcoma
- Hemangioma
- Xanthogranuloma.
REFERENCES:
- Mary Elizabeth Guerra, Savanah D. Gisriel, Emily Christison-Lagay, Matthew A. Hornick,Giant retroperitoneal teratoma in an asymptomatic 6-month-old,Journal of Pediatric Surgery Case Reports,Volume 65,2021,ISSN 2213-5766,https://doi.org/10.1016/j.epsc.2020.101768.
- Jignesh Rathod, Sujan Patel, Ketul S. Barot, Saloni H. Naik, Ravi Bhatt, Jay Chotaliya,
Massive primary retroperitoneal immature teratoma : A case report, International Journal of Surgery Case Reports,Volume 81,2021,ISSN 2210-2612, https://doi.org/10.1016/j.ijscr.2021.105775. - Sarin YK. Peritonitis caused by rupture of infected retroperitoneal teratoma. APSP J Case Rep 2012; 3: 2
Dr VIKHYATH SHETTY
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr SHIKHA JOSHI
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
