

A 76 year old male patient presented with history of right sided chest pain for the past two months
- No H/O cough / shortness of breath / fever.
- No other significant complaints.
FINDINGS:
- A: CT scout image and Contrast enhanced axial image of the thorax
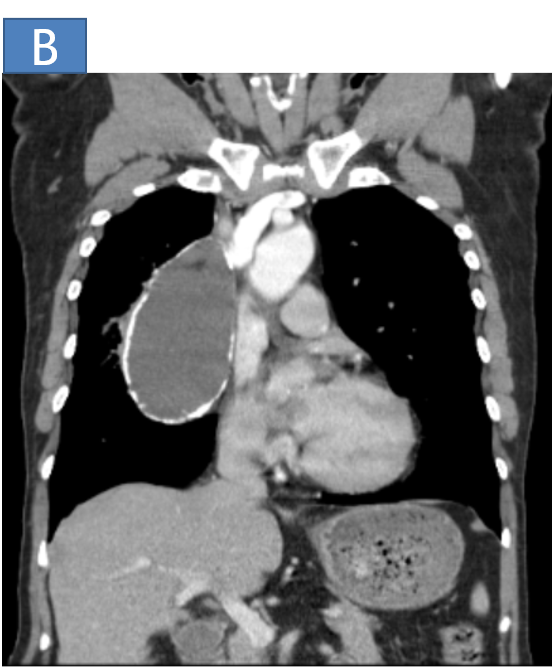
- B: Contrast enhanced CT coronal image of the thorax
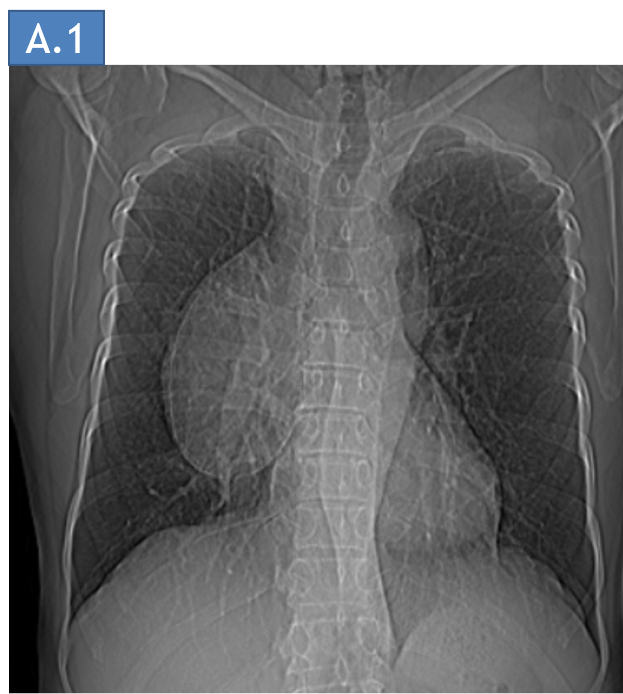
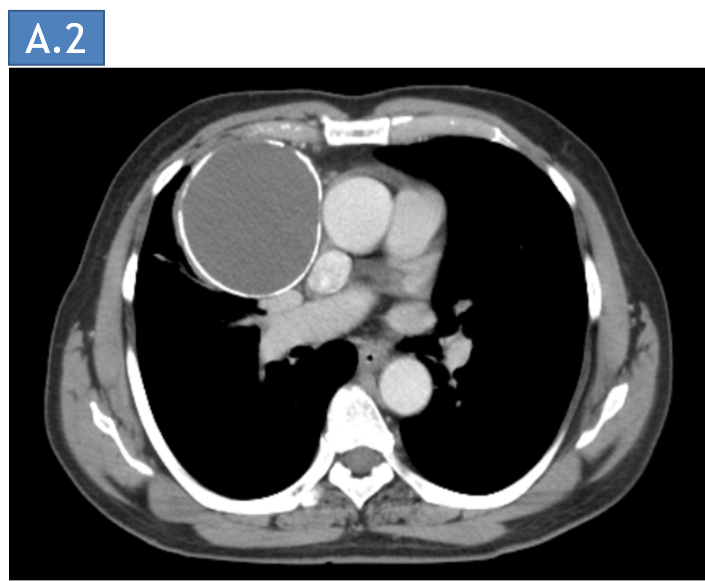
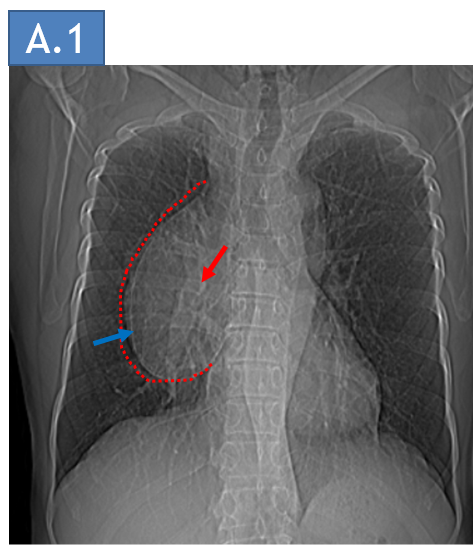
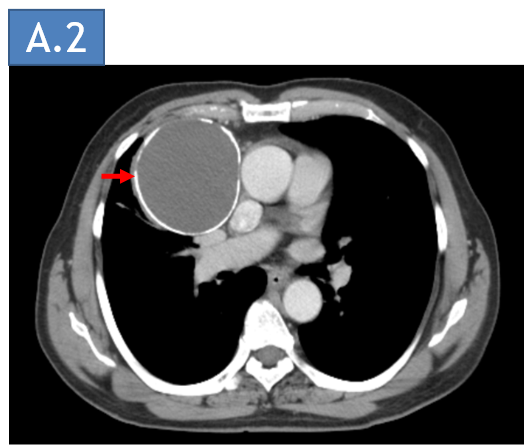
A: CT scout image of the thorax (a.1) and Contrast enhanced axial image of the thorax (a.2)
- Scout image of the thorax showing a large radioopacity silhouetting the right heart border and arch of the aorta (red dotted line). There is a thin rim of calcification is seen within the radiopacity (blue arrow). The pulmonary hilar vessels are seen throught the radioopacity indicating a positive hilum overlay sign(red arrow).
- Axial CECT of the thorax shows a cystic density non enhancing right paracardiac anterior mediastinal lesion(red arrow) just superior to the cardiophrenic angle. The lesion shows thin rim of calcification and is abutting the SVC and the ascending aorta. The lesion is compression the right lung parenchyma.
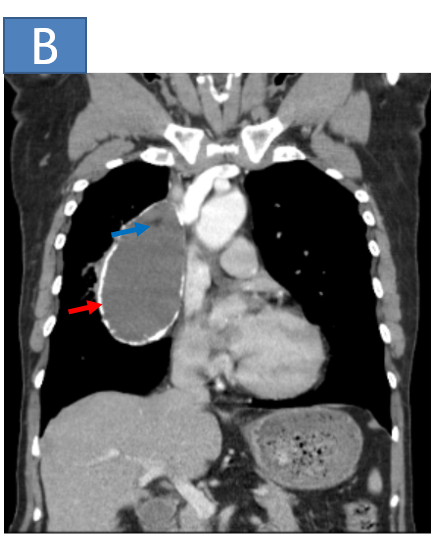
B: Contrast enhanced CT coronal and axial image of the thorax
- Coronal CECT of the thorax shows a cystic density non enhancing right paracardiac lesion (red arrow).
- The lesion shows thin rim of calcification with few fat density areas in the superior aspect of the lesion(blue arrow).
DIAGNOSIS:
- Mature cystic teratoma.
DISCUSSION:
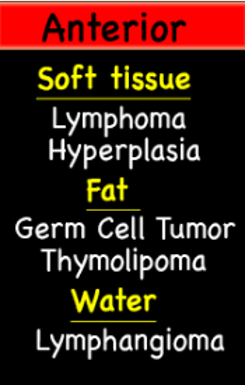
Most common anterior mediastinal masses

Germ cell tumours:
Germ cell tumors are one of the causes of anterior mediastinal mass, and any of the germ cell histologies may be identified. They can therefore be divided histologically into:
Seminoma
Non-seminomatous germ cell tumors (NSGCT)
- Embryonal cell carcinoma
- Choriocarcinoma
- Yolk sac tumor
- Teratoma: most common
- Mixed germ cell tumor
Anterior mediastinal germ cell tumors can be thought of as benign and malignant:
Benign
- Mature teratoma
- Mature teratoma with an immature component of less than 50%.
Malignant
- all others.
It is difficult to distinguish between the various malignant histologies, and clinical correlation with serum tumor markers (AFP, beta-HCG) and biopsy is usually required.
Teratoma:
- The most common mediastinal germ cell tumor, accounting for 50-70%.
- The typical presentation in adults is in the third or fourth decade (the 20s and 30s). In children below one year of age, immature teratomas are common (40%) and may be detected antenatally.
- No particular gender predilection for mature teratomas has been identified (at most there is a slight female predilection). Immature teratomas, however, occur almost exclusively in males.
Imaging features:
Well-demarcated, displacing rather than invading adjacent structures
Usually cystic: 90%
- may be uni- or multiloculated
Septal/rim contrast enhancement
Variable attenuation, consistent with different tissues
- fat
- water density cystic spaces
- fat-fluid levels (specific)
- homogeneous soft-tissue density
- calcification: 26%
- identifiable teeth or bone is seen in up to 8% of cases
Other cystic neoplasms of the anterior mediastinum:
Thymic cyst
- Well-circumscribed, round/oval/saccular, homogeneous mass located near thymic bed
Pericardial cyst
- Well-circumscribed lesion measuring water fluid density with thin or imperceptible walls in the cardiophrenic angle
Lymphoma
- Necrotic, cystic-appearing mediastinal lymph nodes, common finding in newly diagnosed Hodgkin disease
- Multiple markedly enlarged lymph nodes/masses, encasing but respecting vessels
Dr. Deepti H V,
Senior Consultant,
Department of Radiology,
Manipal hospital, Yeshwanthpur, Bengaluru.
Dr. Ram Sanjith V,
Cross Section Fellow,
Manipal hospital, Bengaluru.
