

A 66 year old diabetic and hypertensive lady with one day history of abdominal pain which is progressively increasing in intensity.
Recent history of cough.
On examination:
- Left inferior quadrant tenderness
- Stable vitals
Was advised to undergo CECT
FINDINGS:
- CECT ABDOMEN AND PELVIS
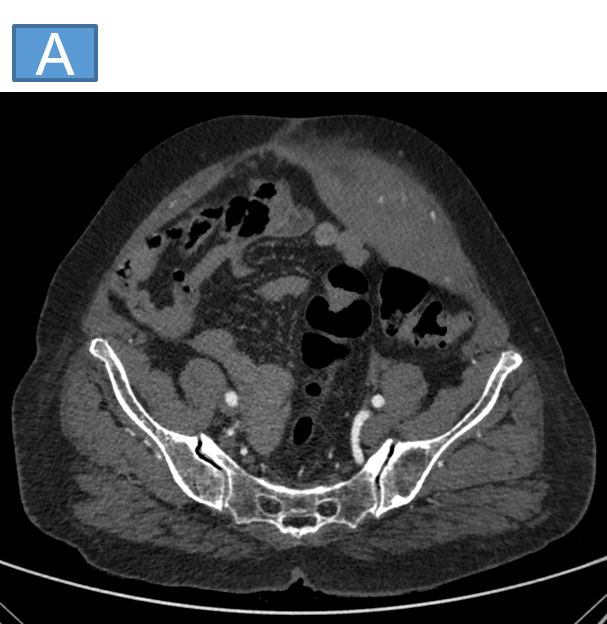


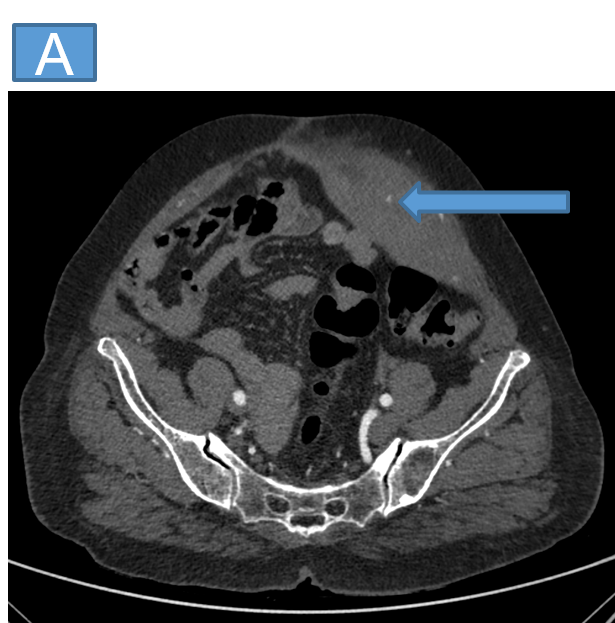
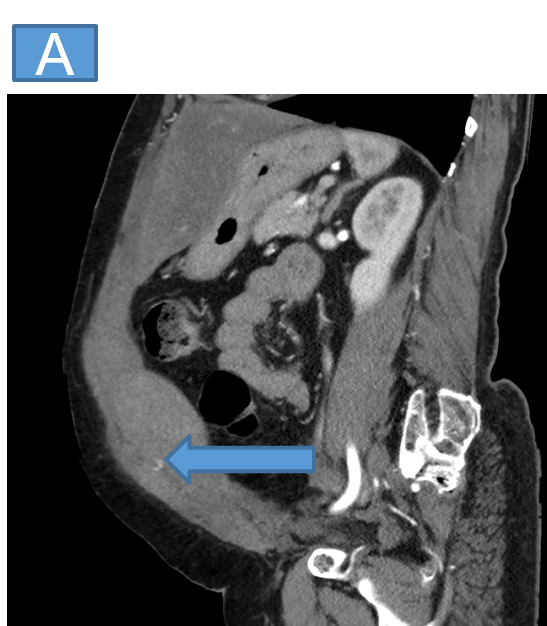
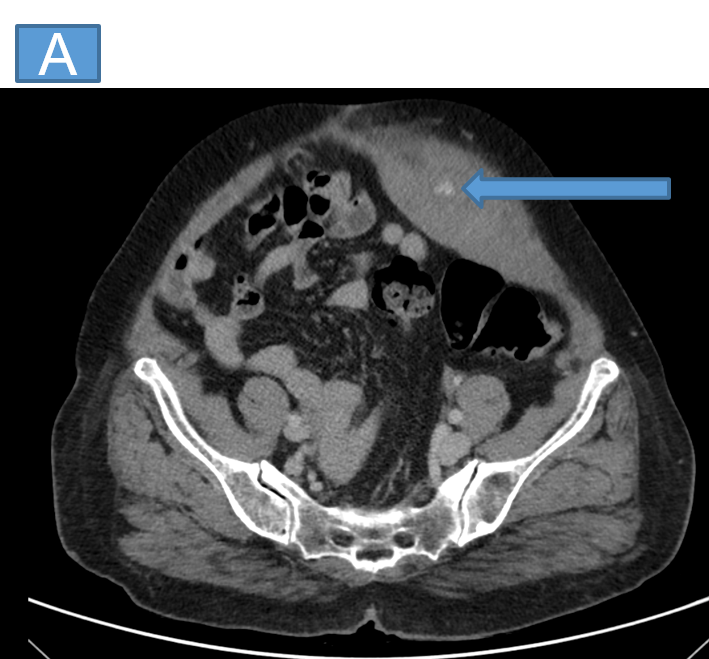
- Axial and sagittal arterial phase images (A and B) show bulky left rectus abdominis muscle appearing diffusely hyperdense suggestive of a haematoma with a tiny speck of contrast blush (arrow).
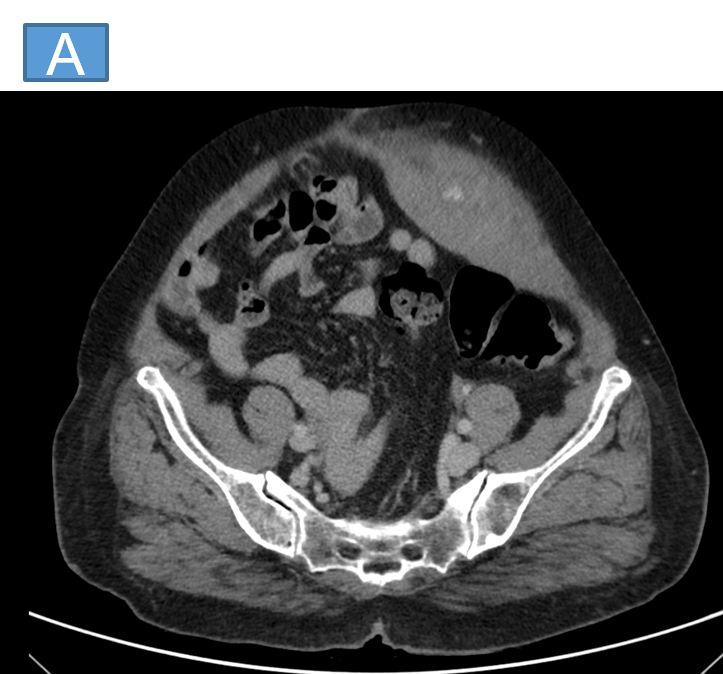
- Subsequent venous axial image shows increase in size and alteration of shape of the contrast blush suggestive of an active bleed.
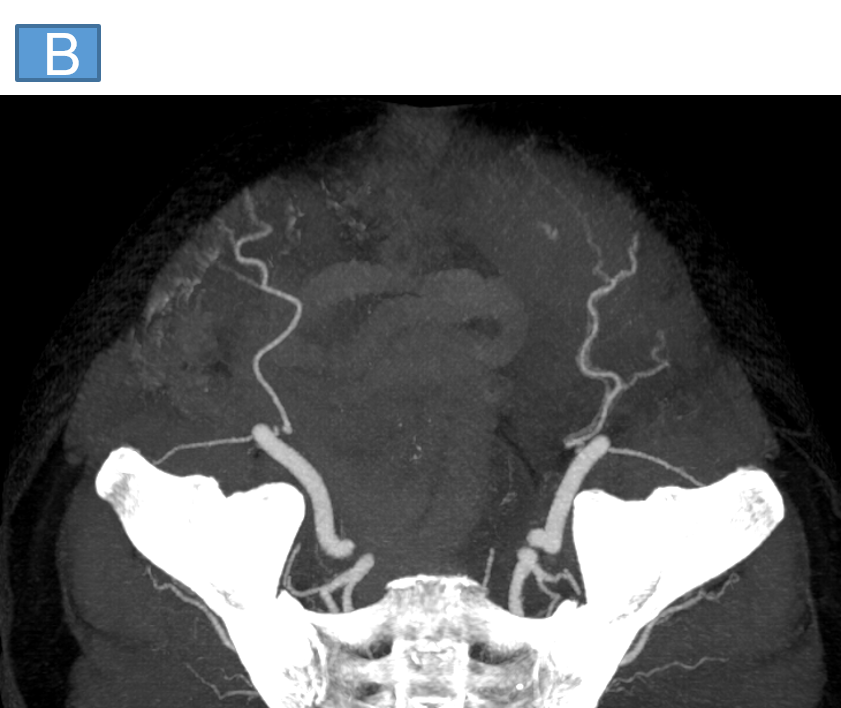
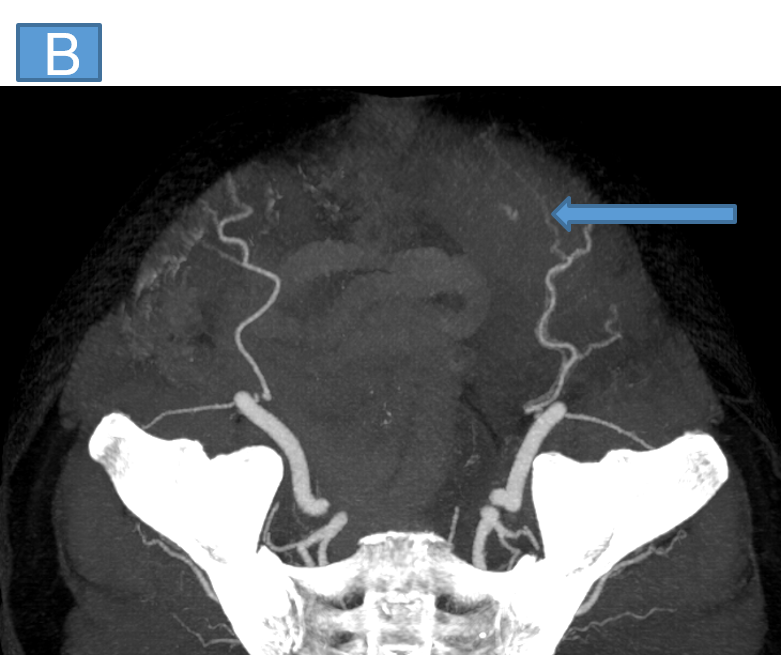
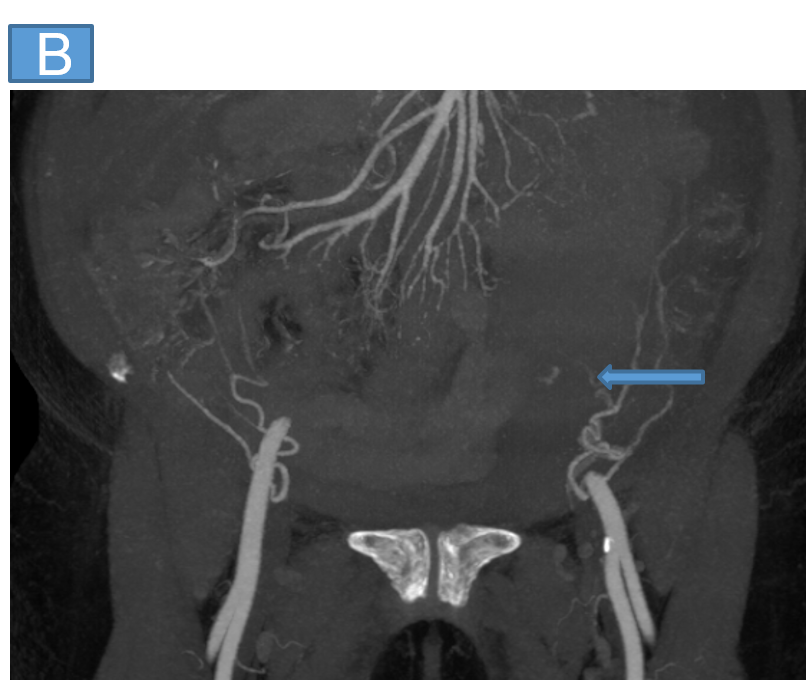
- Axial and coronal MIP images show tortuous left inferior epigastric artery arising from the left external iliac artery with one of the muscular branches (arrows) in close proximity to the area of contrast blush
DIAGNOSIS:
- Spontaneous left inferior epigastric artery injury with abdominal wall haematoma
DISCUSSION:
Inferior epigastric artery (IEA) rupture or damage is not only uncommon but also potentially fatal.
- Causes:- physical injuries to the abdomen, raised intra-abdominal pressure, anticoagulation, and iatrogenic procedures such as percutaneous peritoneal dialysis catheterization, paracentesis trocar placement, surgical drainage, and insertion for laparoscopy.
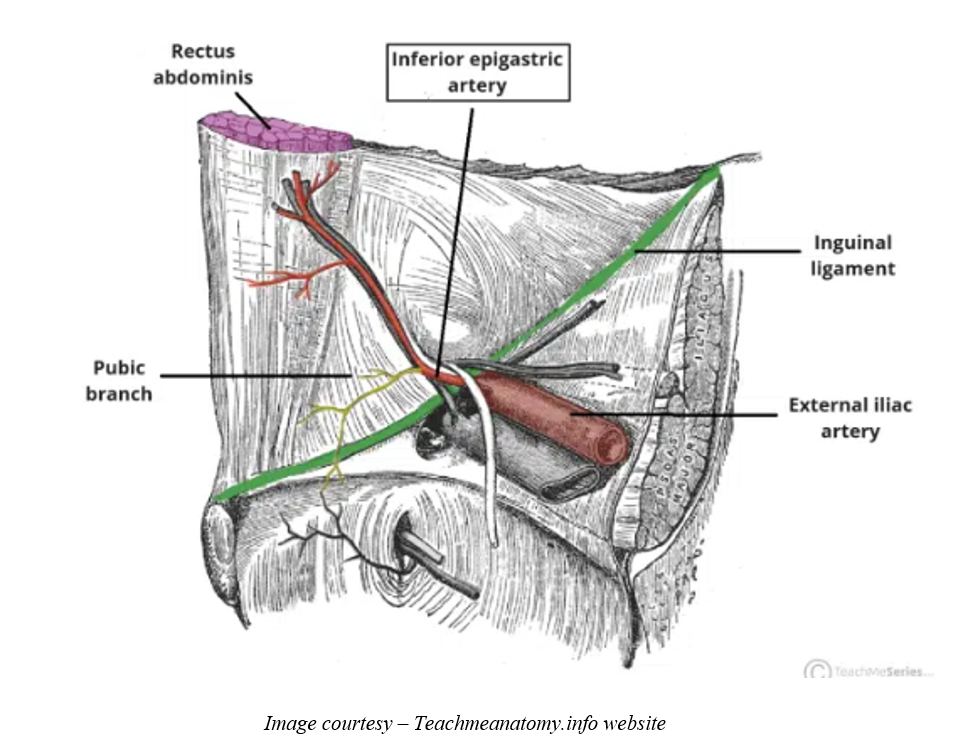
Vascular anatomy if IEA
- Origin:- External iliac artery
- Course:- Ascends in an oblique path passing along the medial border of the deep inguinal ring, it then punctures the transversalis fascia and ascends to enter the rectus sheath just beneath the arcuate line
- Branches:- cremasteric artery, pubic branch and muscular branches
- Termination:- Anastomose with superior epigastric artery
The inferior epigastric arteries are vulnerable to injury because they are situated in a comparatively superficial layer of the abdominal muscle.
Risk factors for spontaneous rectus sheath haematoma:
- coughing, sneezing, straining, twisting, or vomiting that causes the muscle to contract or stretch excessively
- Arteriosclerosis
- Hypertension
- Aging
- Obesity
- Pregnancy
- Prior surgery, trauma, or inflammatory diseases that cause the vessel wall to weaken or reduce muscular resistance
- Conditions that have a propensity to bleed or that call for the use of anticoagulants.
Clinical Presentation
- Acute pain that can mimic peritonitis, incarcerated hernia, ovarian pathology, ruptured abdominal aneurysm, appendicitis,diverticulitis, pancreatitis, periappendicular abscess,ectopic pregnancy
- Late findings: Cullen sign (periumbilical ecchymosis) and Grey Turner sign (flank ecchymosis)
Clinical pointers
- Fothergill sign – hematomas don’t cross midline when patient lifts leg/head in supine position
- Carnett sign – pain and tenderness increases with palpation but remains unchanged on lifting leg/head in supine position
Imaging
- USG – shows hypoechoic areas within the muscle but less sensitive to ascertain extent
- MRI – not routinely used
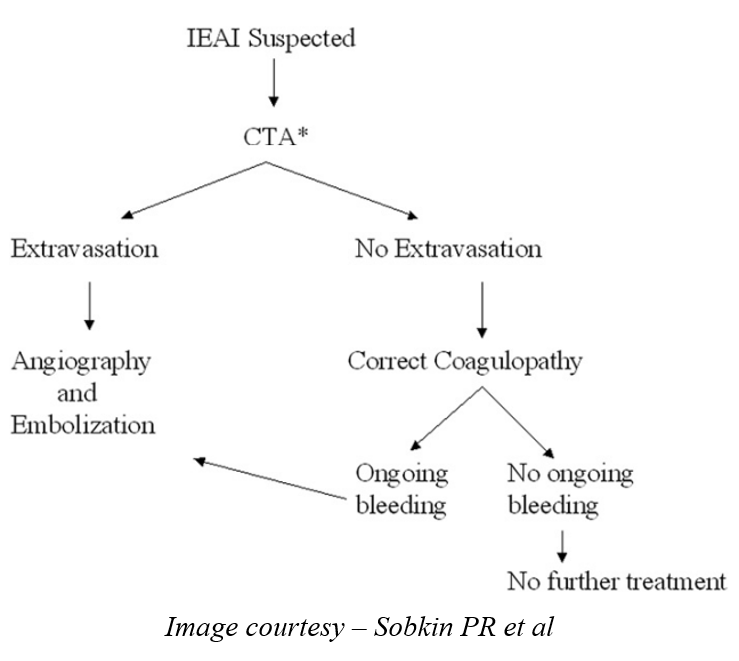
- CT angiography – best modality, can plan management as well with identification of any underlying aetiology
- DSA – gold standard
Prognosis
Usually favourable
Mortality
- 4% in general
- 25% in anticoagulated
Management
Usually conservative
Active bleed/comorbid
- Transarterial embolization - coil/particle
Massive hemorrhage, compartment syndrome, infection - Surgery
References:
- Sobkin PR, Bloom AI, Wilson MW, LaBerge JM, Hastings GS, Gordon RL, Brody LA, Sawhney R, Kerlan RK Jr. Massive abdominal wall hemorrhage from injury to the inferior epigastric artery: a retrospective review. J Vasc Interv Radiol. 2008 Mar;19(3):327-32. doi: 10.1016/j.jvir.2007.11.004. PMID: 18295690.
-
A Case of Rectus Sheath Hematoma with Spontaneous Inferior Epigastric Artery Injury Treated Successfully by Angioembolization, J Korean Soc Emerg Med. 2017; 28(4): 391-394.
DR RAJESH HELAVER
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr RAHUL KARTHIK LINGUTLA
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr ANAGH VISHNU NARAYANAN
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
