
A 64-year-old presenting with abdominal pain and vomiting. History of a lesion in the left heel for 2 years and left inguinal region swelling for 6 months.
A 64-year-old presented with abdominal pain and vomiting. History of a lesion in the left heel for 2 years and left inguinal region swelling for 6 months.
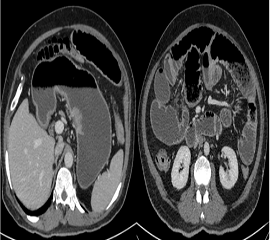
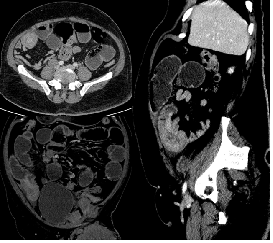
- CECT Abdomen and Pelvis demonstrates dilated stomach and small bowel loops with air-fluid levels and positive small bowel faeces sign. An endophytic lesion along the lesser curvature of stomach. Transition point in right lower quadrant, where there is ileo-ileal intussusception with a small bowel metastatic lesion acting as lead point.
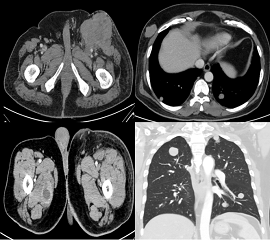
- CECT Chest, Abdomen and Pelvis demonstrates widespread metastatic lesions in left inguinal nodal mass, chest wall lesion, multiple pulmonary nodules and intramuscular lesion in right adductor magnus.
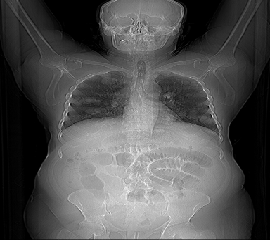
- Topogram demonstrates multiple cannon ball metastatic lesions and central dilated bowel loops.
- Biopsy of left inguinal mass suggestive of metastatic lesion of malignant melanoma.
- Malignant melanoma of left foot with extensive metastases and acute small bowel obstruction secondary to ileo-ileal intussusception with a small bowel metastatic deposit as a lead point.
DISCUSSION:
- Malignant melanoma is an aggressive neoplasm that arises from
melanocytes, which predominantly occur in the basal layer of the
the epidermis of the skin. - The thorax is the most common site of metastases in malignant
melanoma. - The small bowel is the most common site of the gastrointestinal tract
involvement by metastatic melanoma, hence are a risk factor for
intussusception. - Metastases to skeletal muscle are uncommon.
Differential diagnosis:
- Primary neural tumours such as schwannomas.
- Invasive fungal infections such as aspergillosis or mucormysosis (in severely immunocompromised individuals).
- Meningeal inflammatory disorders such as sarcoidosis or histiocytosis.
REFERENCES:
- Fishman EK, Kuhlman JE, Schuchter LM, Miller JA et al. CT of malignant melanoma in the chest, abdomen, and musculoskeletal system. Published Online Jul 1 1990. doi.org/10.1148/radiographics.10.4.2198632
- Patnana M, Bronstein Y, Szklaruk J, Gershenwald JE. Multimethod imaging, staging, and spectrum of manifestations of metastatic melanoma. Published January 11, 2011. doi.org/10.1016/j.crad.2010.10.014
- Keraliya AR, Krajewski KM, Braschi-Amirfarzan M, et al. Extracutaneous melanomas: a primer for the radiologist. Insights Imaging. 2015;6(6):707-717. doi:10.1007/s13244-015-0427-8
Dr. Diwakar C
Radiology Resident,
Manipal Hospitals Radiology Group
Dr. Anita Nagadi
MD, MRCPCH (UK), FRCR (UK), CCT (UK)
Senior Consultant Radiologist
Manipal Hospitals Radiology Group.