
A 61-year- old male with c/o paraesthesia in both lower limbs x 2 years, upper limbs x 1 year, occasional difficulty in gripping pen while writing
- 61-year- old Male.
- C/o paraesthesia in both lower limbs x 2 yrs , Upper limbs x 1 year
- The occasional difficulty in gripping pen while writing.

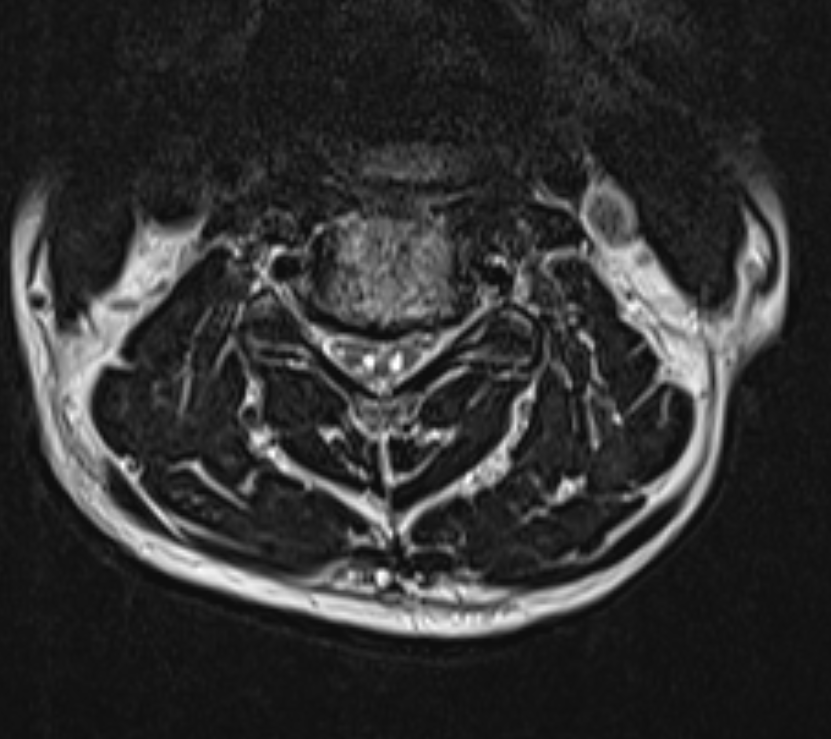
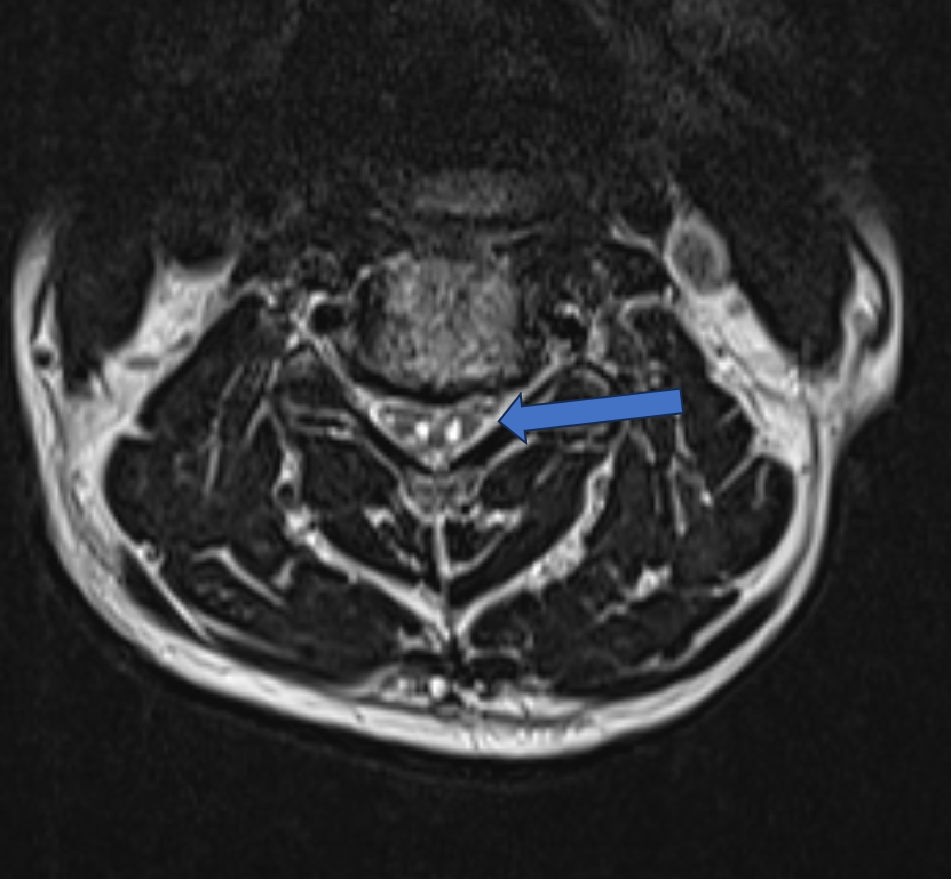
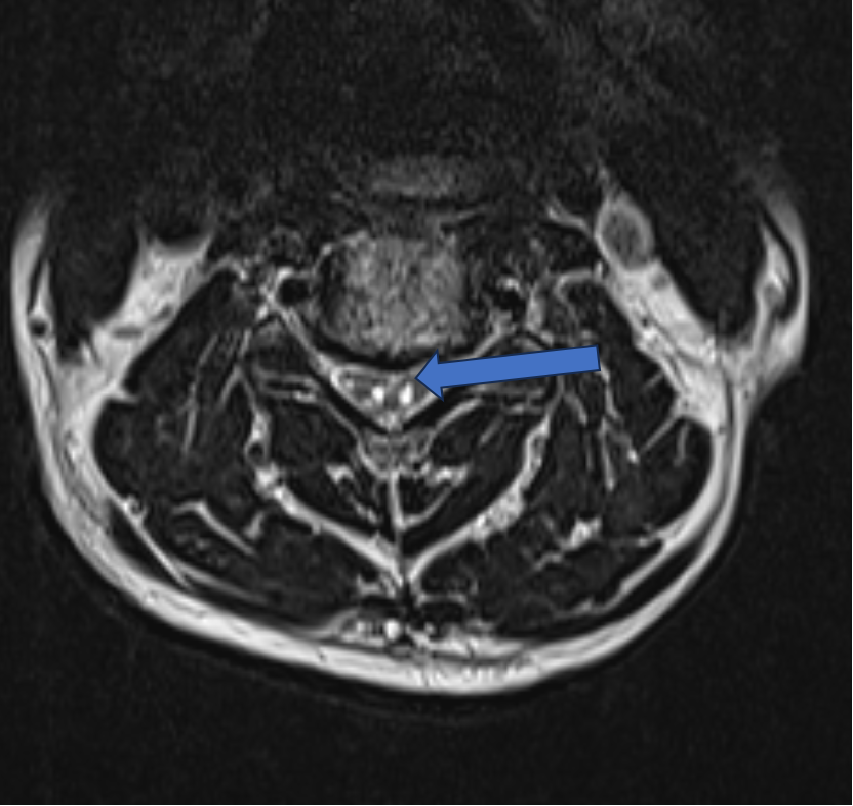
- Axial T2 W Image – Posterior disc osteophyte complex noted at C4 – C5 level indenting ventral thecal sac and Two symmetrical high signal foci in anterior spina cord – owl-eyes sign, also known as snake-eyes sign or fried-eggs sign.
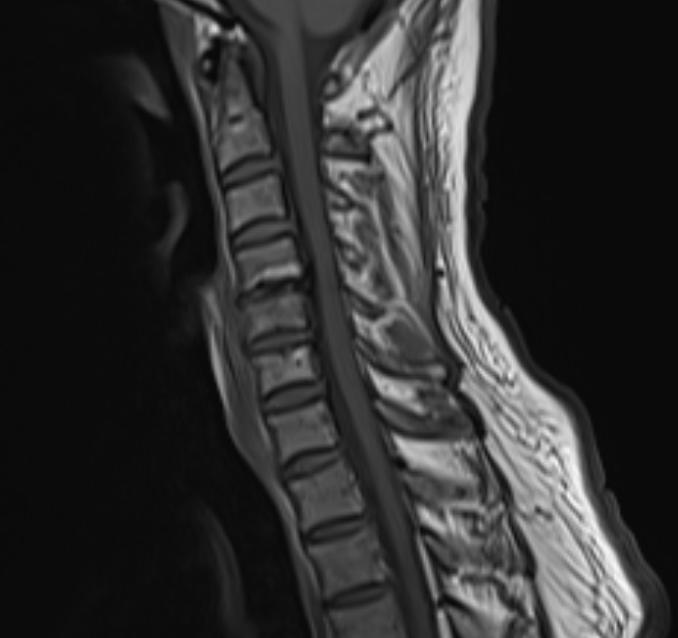
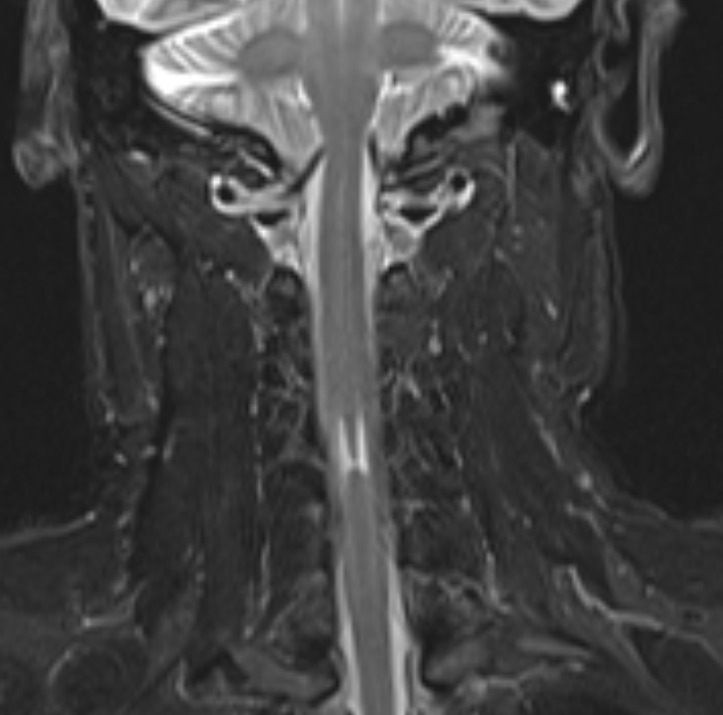
- The sagittal T2 W image shows is a “pencil-like” vertical linear high T2-weighted signal.
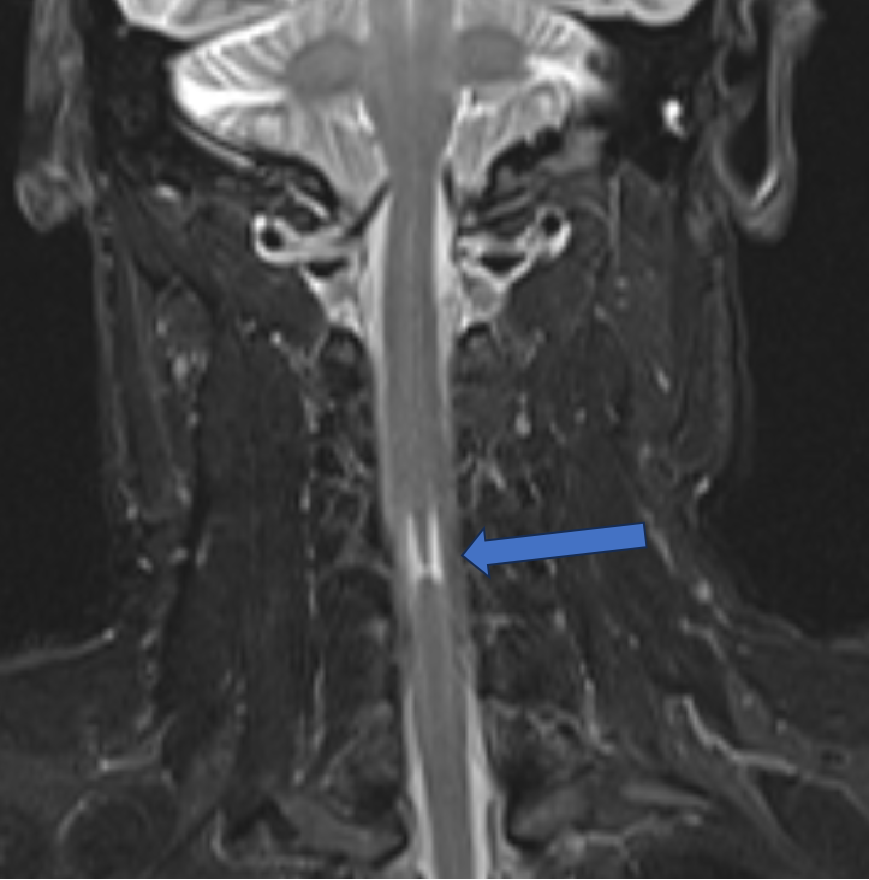

Diagnosis: Chronic compressive myelopathy.
Radiographic featuresMRI:
- High T2 signal intensity in a anterior part of compressed segment relative to a non-compressed segment.
- Administration of contrast is helpful in excluding other causes such as spine infection, tumor, demyelinating disease, and vascular malformations. However, gadolinium enhancement is present in 7.3% of cervical myelopathy cases.
Discussion:
- Compressive myelopathy refers to neurological deficits that result from compression of the spinal cord.
It most commonly occurs in the cervical spinal cord.
Pathology - Any cause of spinal canal stenosis including cervical spondylosis (endplate changes, disc herniation , osteophytes , facet joint arthropathy, ligamentum flavum hypertrophy) , spinal osteochondroma , extra dural mass , paravertebral ligamentous ossification, and congested epidural vein , Cervical spondylosis frequently causes chronic myelomalacic changes of the spinal cord and rarely causes acute spinal cord edema.
- The Owl’s Eyes Sign has been used as a descriptive term in several reports since the advent of MR imaging and is most often thought of as a sign of cord infarction following occlusion of the anterior spinal arteries. The term Owl’s Eyes was perhaps first used by Mawad in 1990 but the “sign” was clearly demonstrated on MR in a case reported by Kulkarni in 1987.
- In fact it is a non-specific sign and not pathognomonic of infarction but can occur with a number of insults to the spinal cord including remote cord contusion, chronic compressive myelopathy, infection and inflammation.
Differential diagnosis:
- Anterior spinal artery ischemia.
- Chronic compressive myelopathy.
- Amyotropic lateral sclerosis.
- Neuromyelitis optica.
- Poliomyelitis like syndrome.
- Hopkins syndrome.
- Spinal muscular atrophy.
REFERENCE:
- Ghosh PS, Mitra S. Owl’s eye in spinal magnetic resonance imaging. Archives of neurology. 2012 Mar 12;69(3):407-8.
- Udiya AK, Shetty GS, Singh V, Phadke RV. Owl eye sign”: anterior spinal artery syndrome. Neurol India. 2015 May 1;63(3):459.
- Fontanella MM, Zanin L, Bergomi R, Fazio M, Zattra CM, Agosti E, Saraceno G, Schembari S, De Maria L, Quartini L, Leggio U. Snake-eye myelopathy and surgical prognosis: case series and systematic literature review. Journal of Clinical Medicine. 2020 Jul 12;9(7):2197.Ramineni KK, Kandraju SS, Jakkani RK, Alwala S. Imaging highlights of anterior spinal cord infarction: Owl’s eye sign. Curr J Neurol. 2021 Apr 4;20(2):118–9. doi: 10.18502/cjn.v20i2.6749. PMCID: PMC8743178.
- Tallapalli AV, Nashi S, Shrivastava M, Rajendran S, Kulkarni GB, Alladi S. An Imaging Clue for Diagnosis of Spinal Cord Infarct. Neurology India. 2022 Jul 1;70(4):1760.
Case Contributors:
Dr. Harsha chadaga
Senior Consultant and Head of Radiology
Manipal Hospitals Radiology Group (MHRG)
Dr. Nikita Patel
Cross-sectional fellow
Manipal Hospital, Yeshwanthpur, Bengaluru
