
A 57-year-old male with atypical angina and a history of recurrent syncope episodes for 1 year
- A 57-year-old male with atypical angina and a history of recurrent syncope episodes for 1 year.
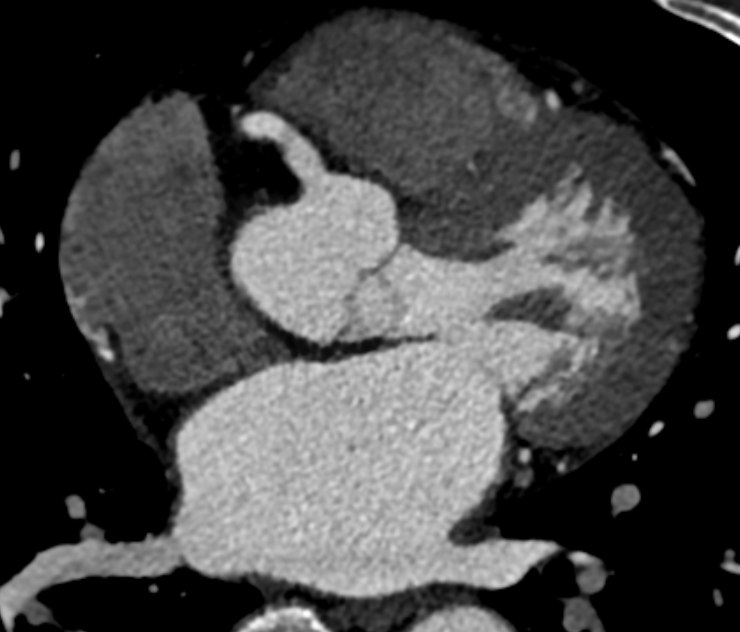
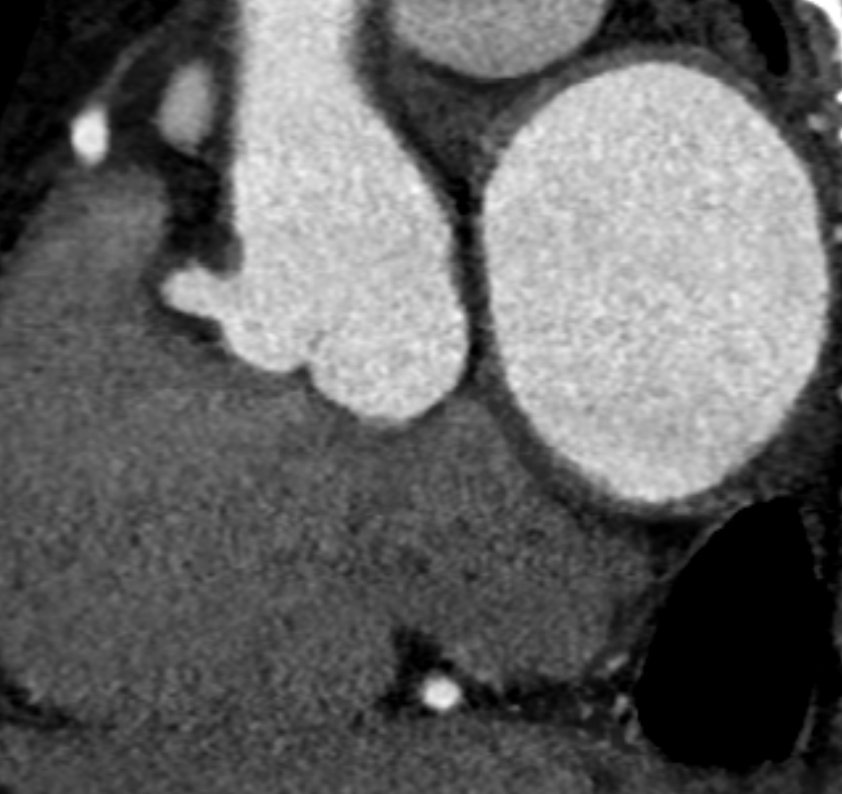
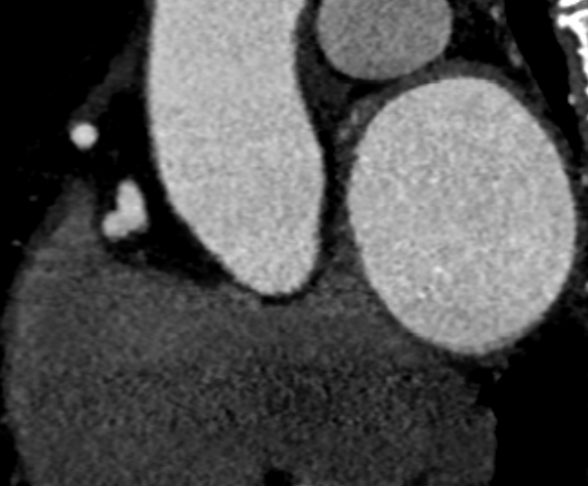
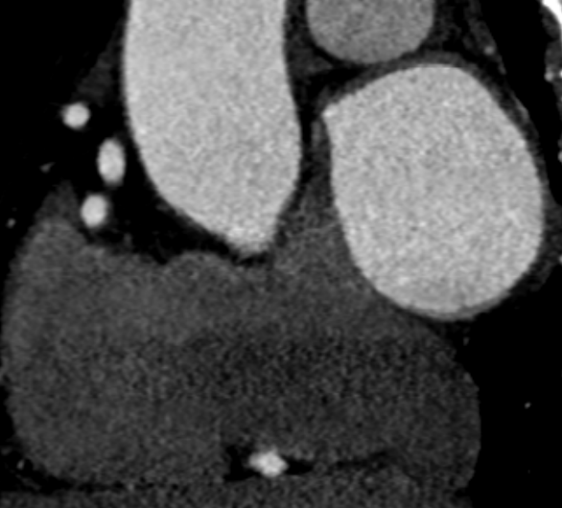
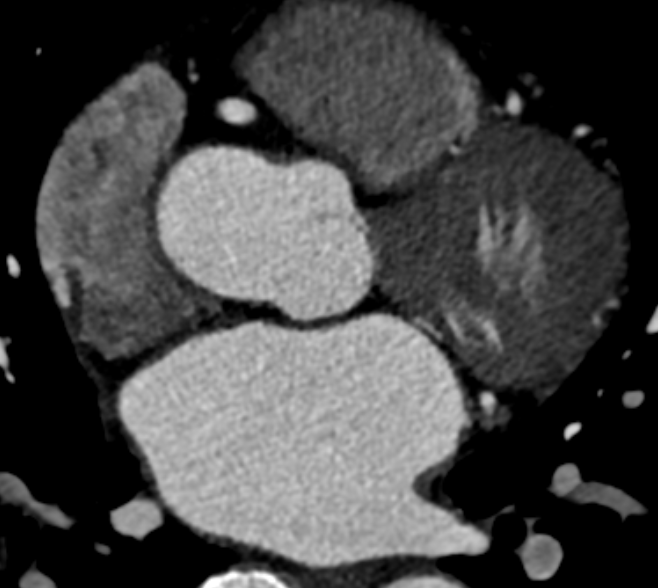
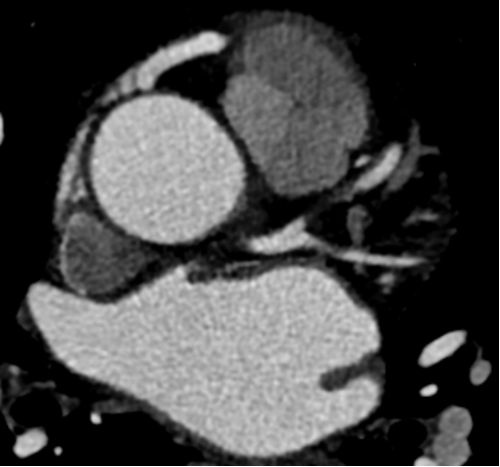
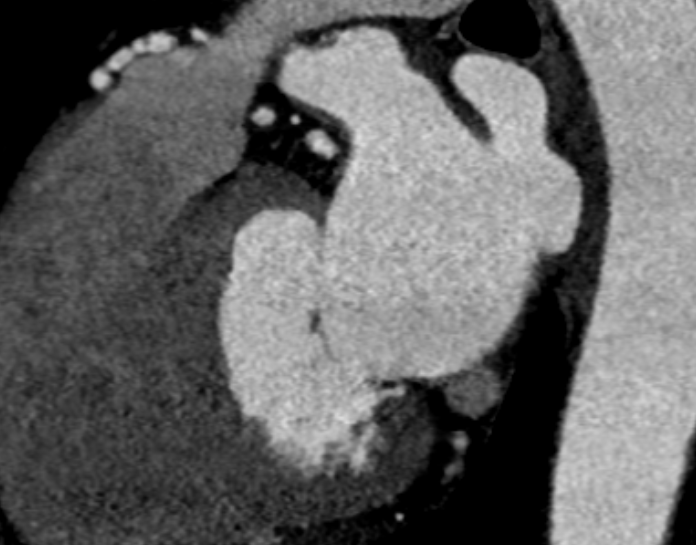
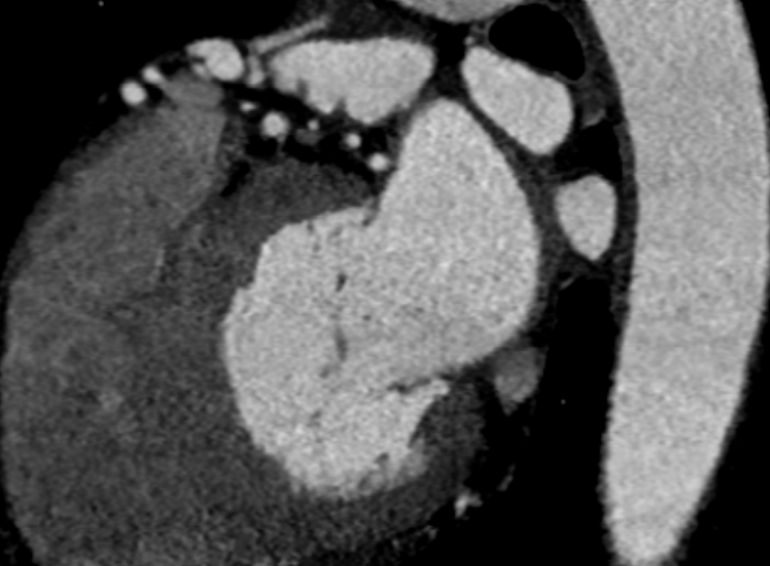
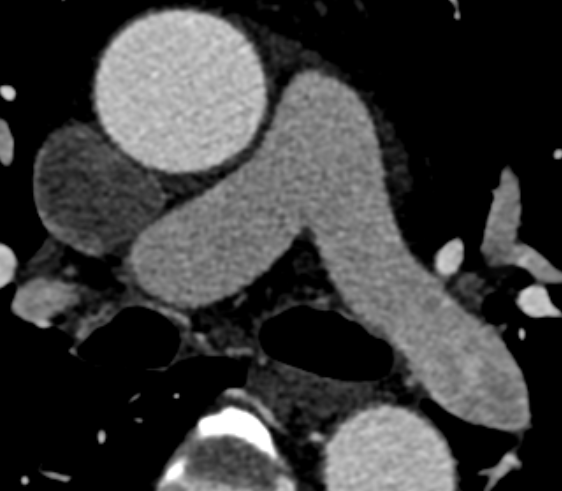
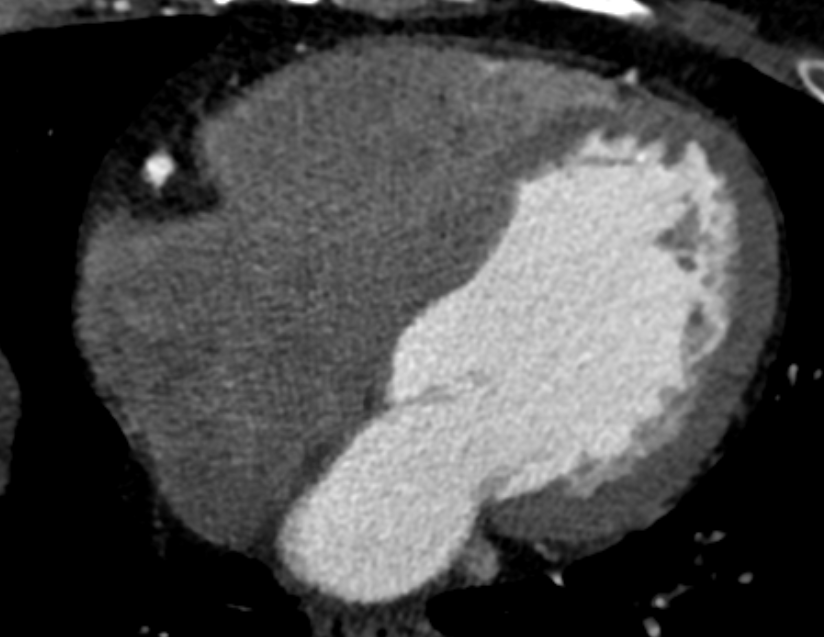
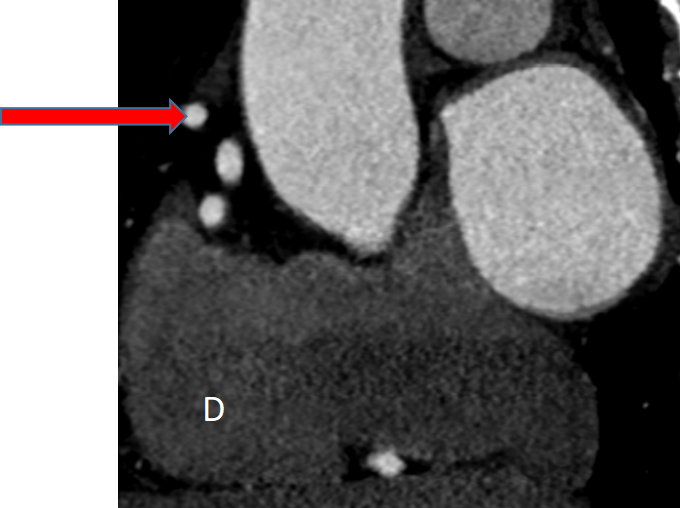
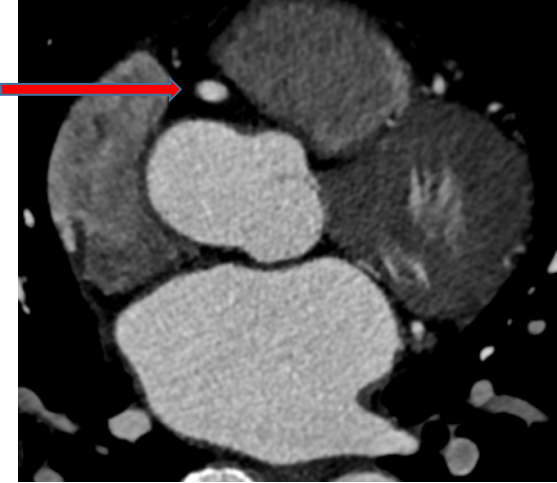
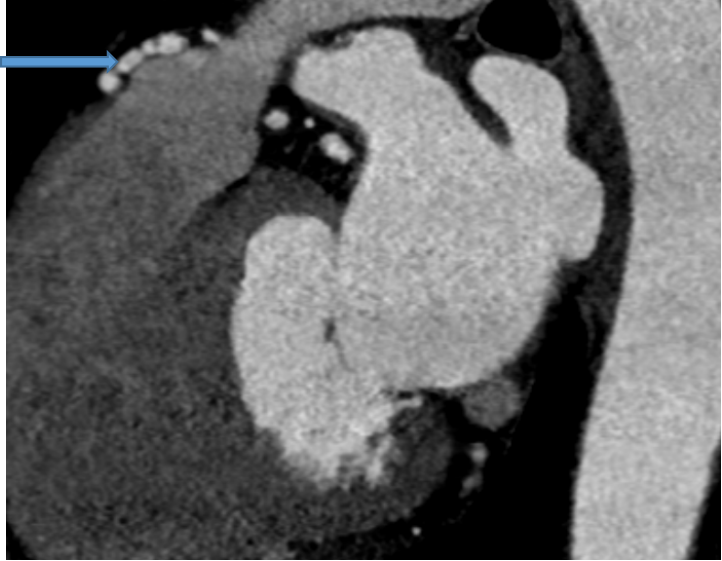
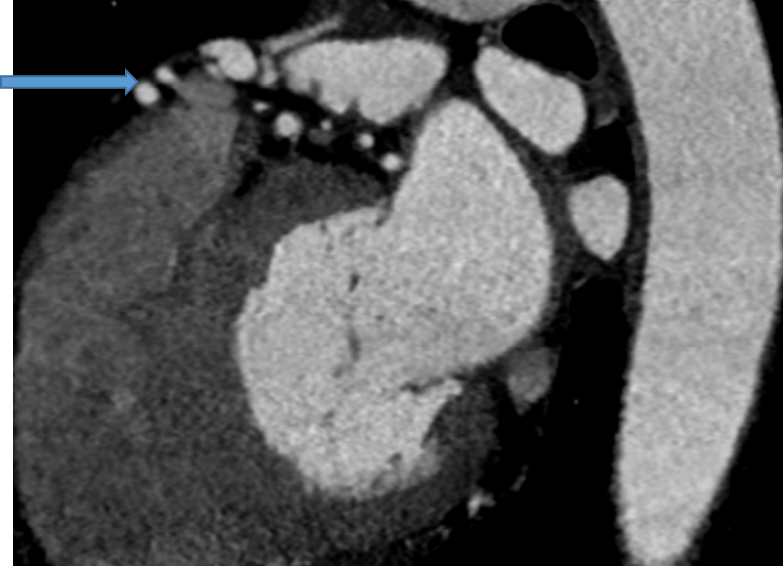
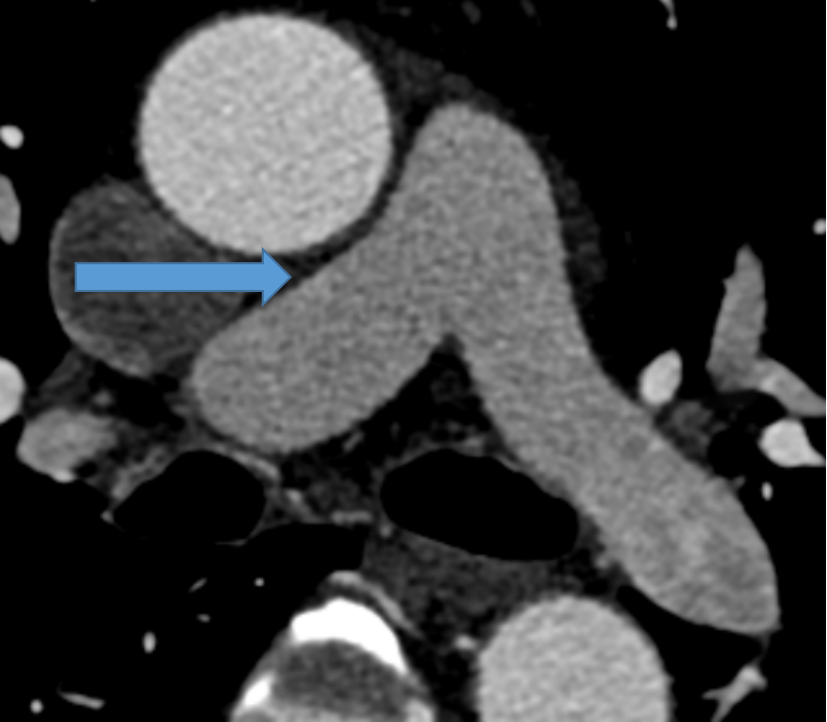
- A and B) shows normal origin of right coronary artery from the right coronary sinus C and D) shows an anomalous prominent artery arising from the proximal right coronary artery (red arrow)
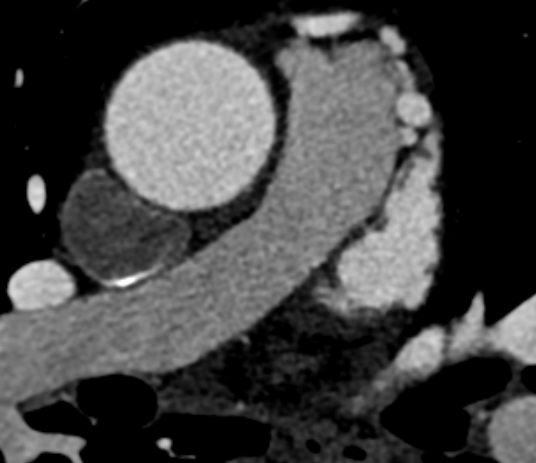
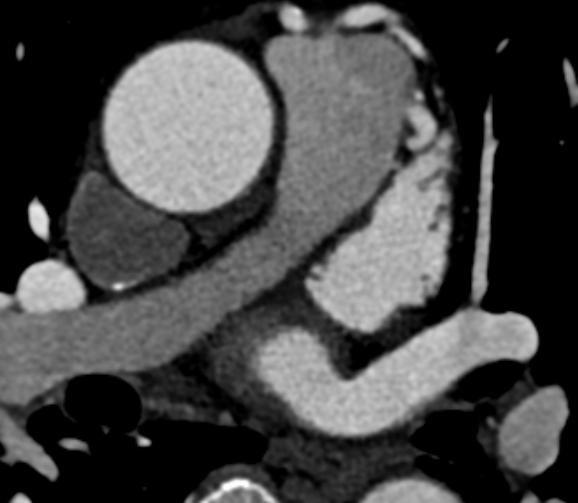
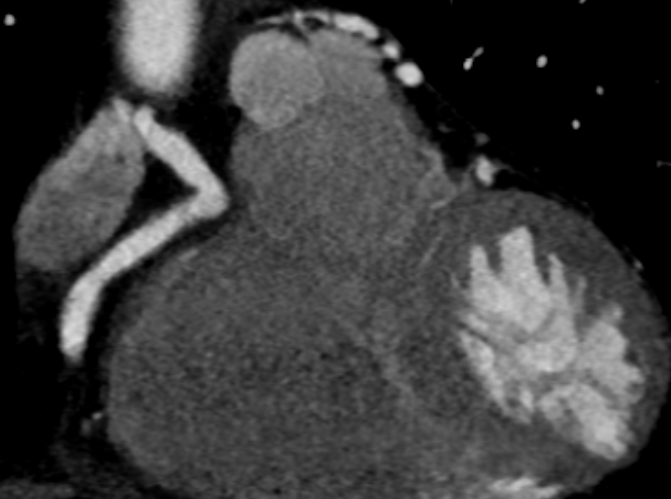
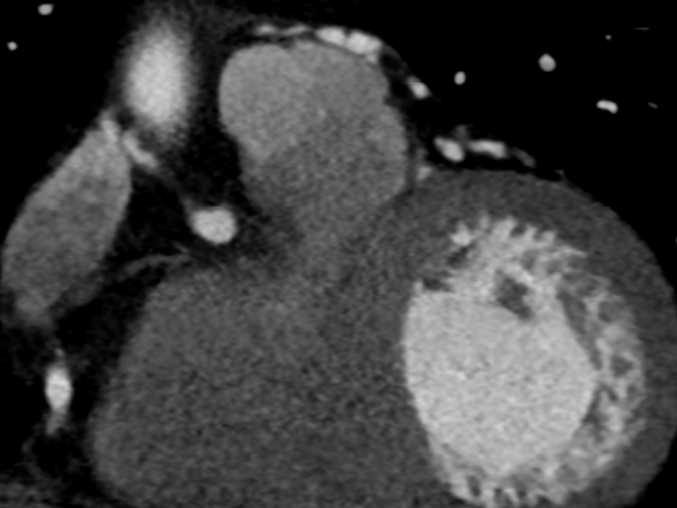
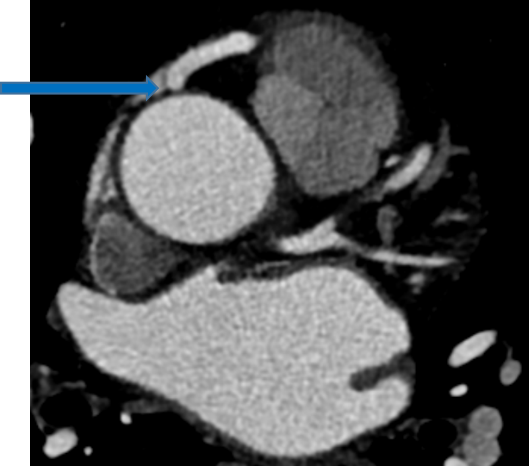
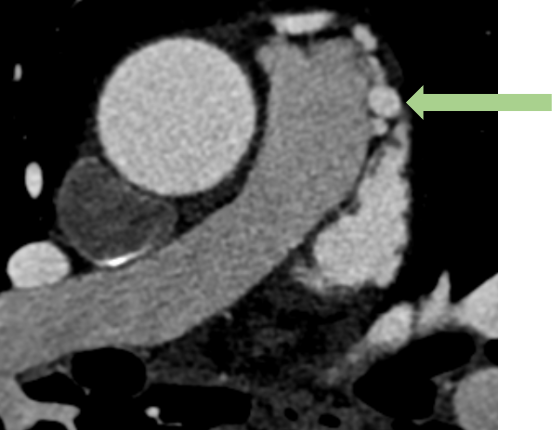
- Serial axial CECT coronary angiogram images show the anomalous prominent artery with a tortuous course (red and blue arrows), crossing over the right ventricular outflow tract. The distal part divides into multiple collaterals, communicating with the main pulmonary artery trunk on the left side (green arrow)
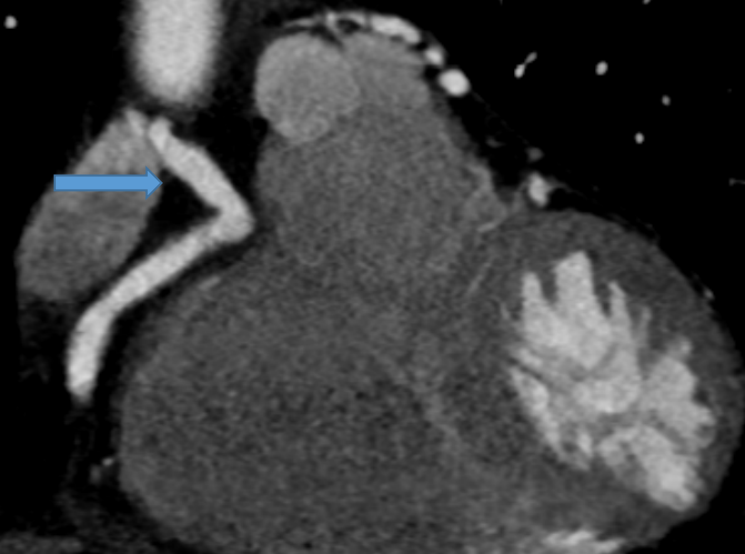
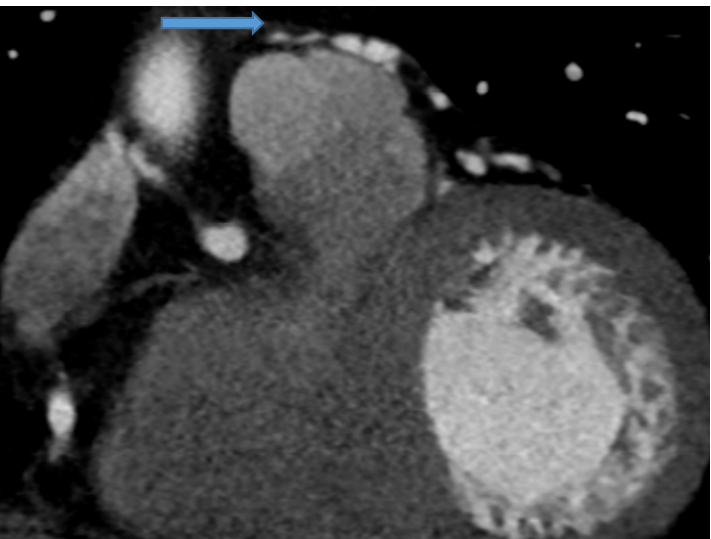
- Sagittal CECT coronary angiogram images show the anomalous prominent artery coursing anterosuperiorly and draining into the distal main pulmonary artery (blue arrows)
- Coronal CECT coronary angiogram images show an anomalous prominent artery draining into the distal main pulmonary artery (blue arrow)
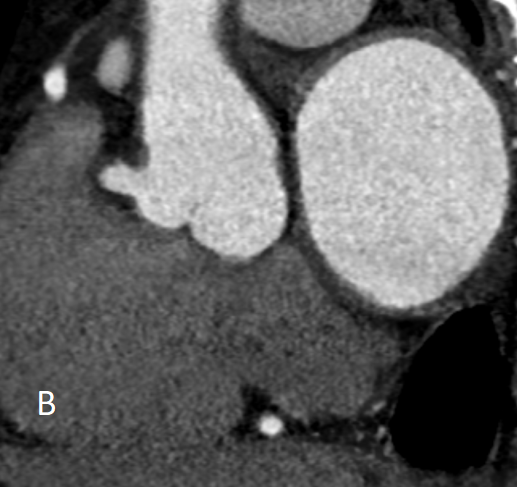
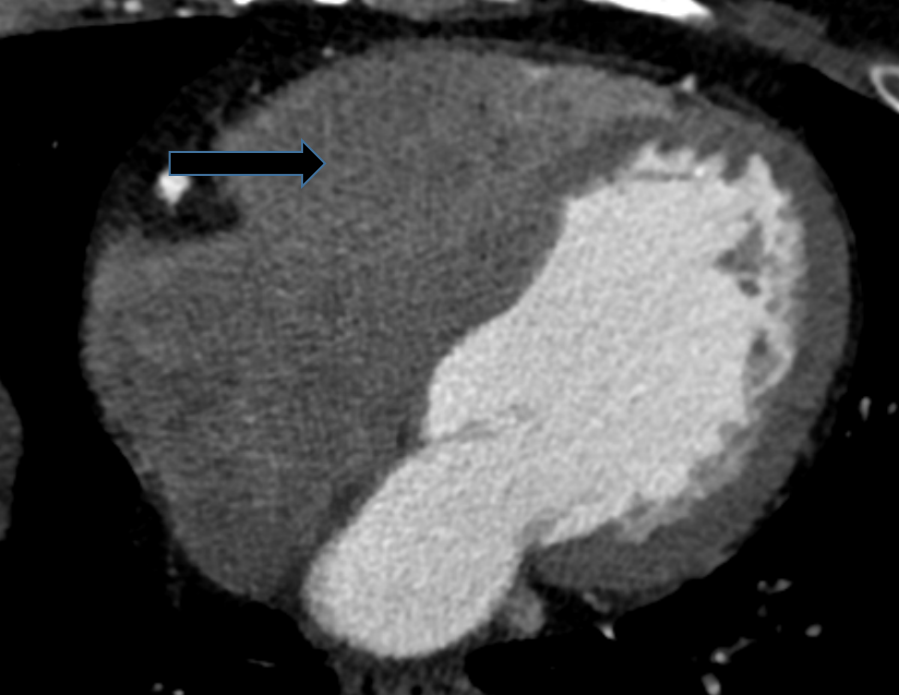
- Axial CECT coronary angiogram showing early opacification of contrast in the main pulmonary trunk, right and left pulmonary artery (blue arrow). No significant contrast seen in right ventricle(black arrow).
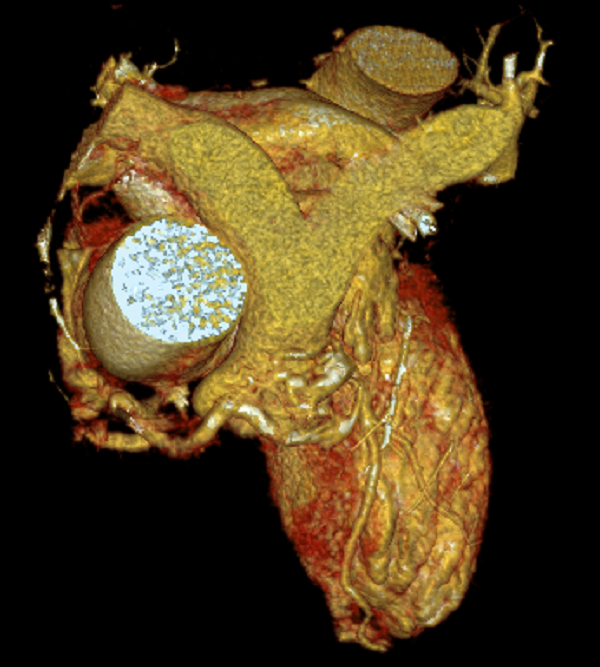
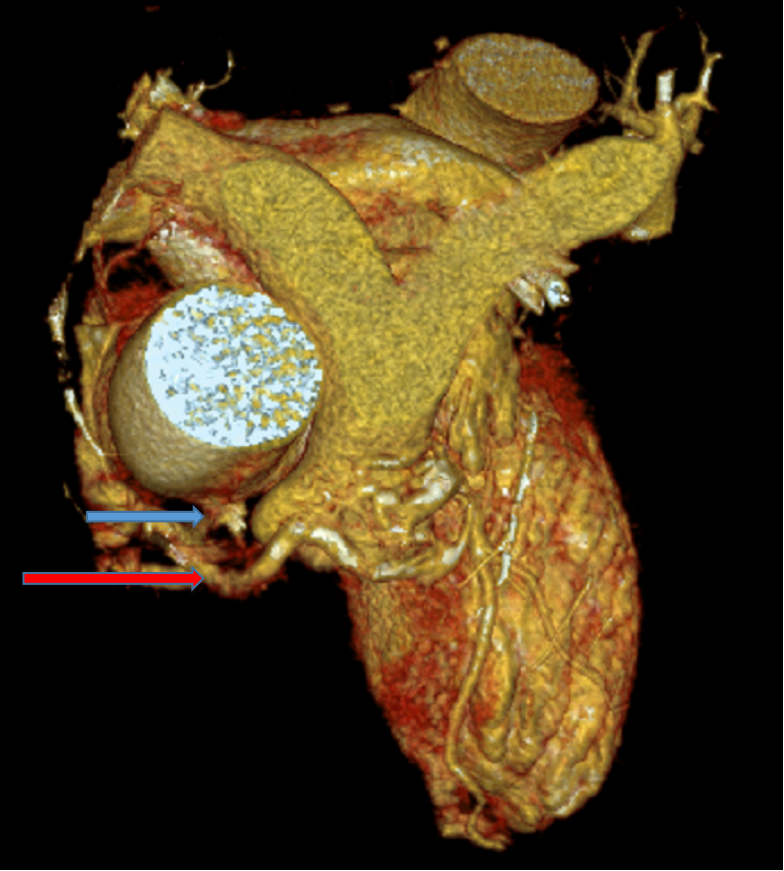
- VRT image showing the fistulous vascular (red arrow) communication of the RCA (blue arrow) and pulmonary artery (green arrow)



Diagnosis:
- Anomalous fistulous communication of right coronary artery with main pulmonary trunk with coronary steal.
Discussion:
Coronary Artery to Pulmonary Artery Fistula (CPAF):
- Definition:
A type of coronary arteriovenous fistula characterized by an abnormal connection between a coronary artery and either a pulmonary artery or the pulmonary trunk. - Pathogenesis:
Rooted in the Hackensellner involution-persistence hypothesis, wherein normal development sees only two of six aortic sinus branches persisting to form coronary arteries. A failure in this involution process results in the formation of a coronary-to-pulmonary artery fistula. - Clinical Consequence:
Left-to-right shunts occur, leading to a coronary steal phenomenon and subsequent myocardial ischemia. Pharmacological Stress testing like employing adenosine or dipyridamole stress testing is used for diagnosis.
Associations with CPAF:
- Coronary Artery Aneurysms:
Present in approximately 20% of cases. - Pediatric Associations:
Commonly associated with:- Pulmonary atresia (abnormal pulmonary valve).
- Ventricular septal defects (VSDs).
Location:
- Coronary Arteries Involved:
- Most Common: Left-main or left anterior descending artery.
- Second Most Common: Right coronary artery.
- Pulmonary Arterial Vessel:
Most commonly involves the main pulmonary artery.
Subtypes:
- Single Prominent Fistulous Connection:
Typically between the Left Anterior Descending (LAD) or Right Coronary Artery (RCA) and the main pulmonary trunk. - Multiple Small-Caliber Fistulous Connections:
Arising from the LAD or RCA, these connections may drain into the main pulmonary trunk or the broader pulmonary arterial system.
Treatment Option for CPAF with Coronary Steal:
- Revascularization:
- Consider surgical intervention or percutaneous transcatheter closure to correct the abnormal connection, addressing coronary steal and restoring normal blood flow.
- Percutaneous transcatheter closure for cases with a high perioperative risk, proximal fistulas, and a single drainage site.
- Medical Therapy:
Use nitroglycerin and vasodilators to alleviate symptoms related to coronary steal. - Lifestyle Modifications:
Advocate heart-healthy habits: diet, exercise, and smoking cessation. - Close Monitoring:
Regularly monitor symptoms and conduct follow-up assessments to adjust the treatment plan as needed.
Differential Diagnoses:
- Coronary Arteriovenous Fistula:
- Involves abnormal connections between coronary arteries and veins.
- Imaging characteristics may resemble those of CPAF, sharing the common feature of abnormal vascular connections.
- Aortic-Pulmonary Window Anomalies:
- Anomalies affecting the aortic-pulmonary window, like aortic-pulmonary septal defect.
- Can present with abnormal communications between the aorta and pulmonary artery, and imaging features may overlap with those of CPAF.
- Coronary Artery Anomalies:
- Various congenital anomalies of the coronary arteries, such as ARCAPA (Anomalous right coronary artery from pulmonary artery).
- Arises due to the improper implantation of the coronary artery on the pulmonary artery.
References:
- Congenital Coronary Artery–to–Pulmonary Artery Fistula with Anomalous Origin of Right Coronary Artery from Pulmonary Artery: A Case of “Double Trouble”, Parveen Kumar, Radiology: Cardiothoracic Imaging 2021 3:4.
- Funabashi N, Kobayashi Y. Clinical manifestation of coronary pulmonary arterial fistula diagnosed by cardiac computed tomography. European Heart Journal. 2022 Feb 1;43(Supplement_1):ehab849-114.
Dr. Faizel Abdul Khader
Consultant Radiologist
MHRG
Dr.Farhin Mushthiri A
DNB Radiology Resident
MHRG
