
A 53 year old male, with history of previous left nephrectomy and right iliac fossa pain.
FINDINGS:
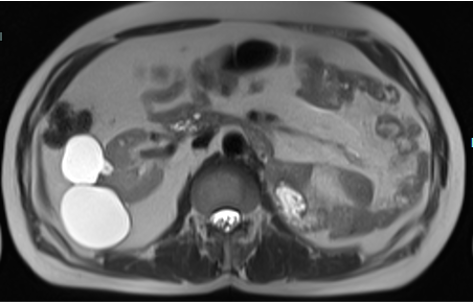
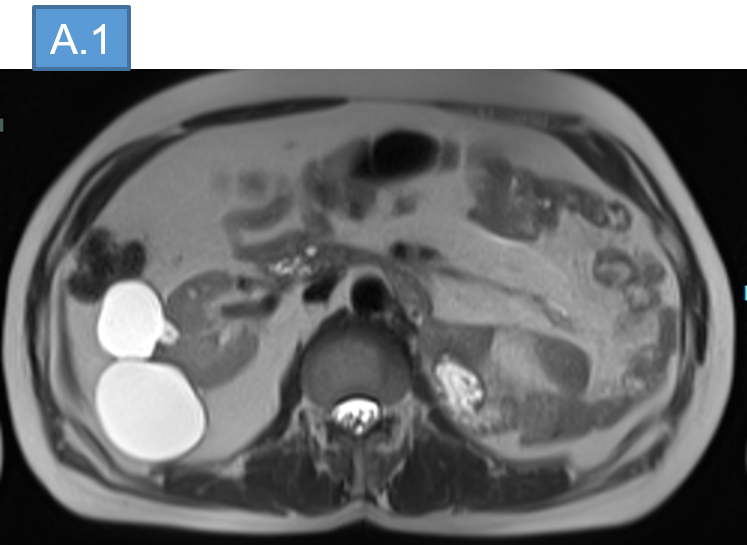
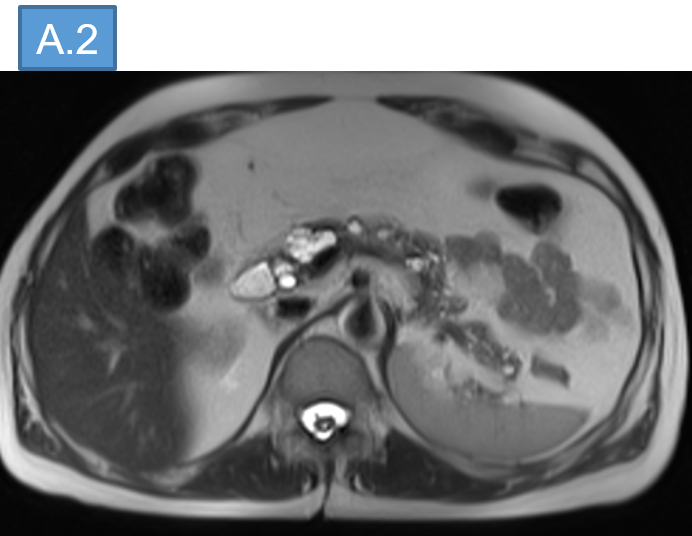
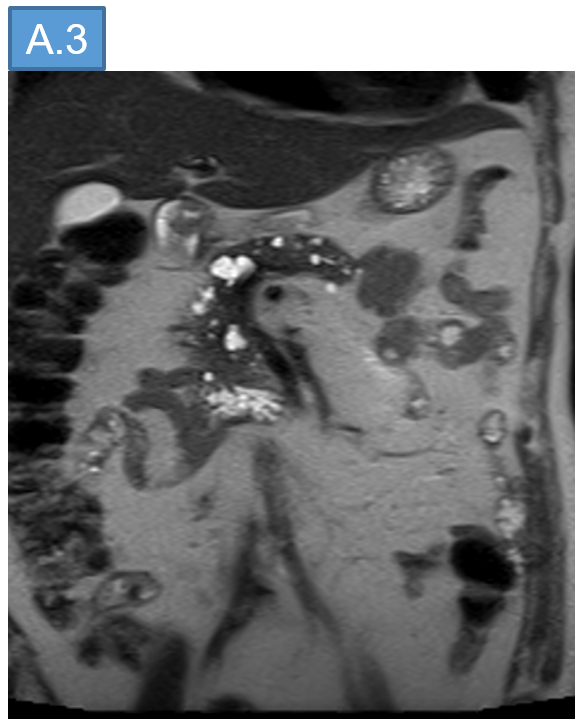
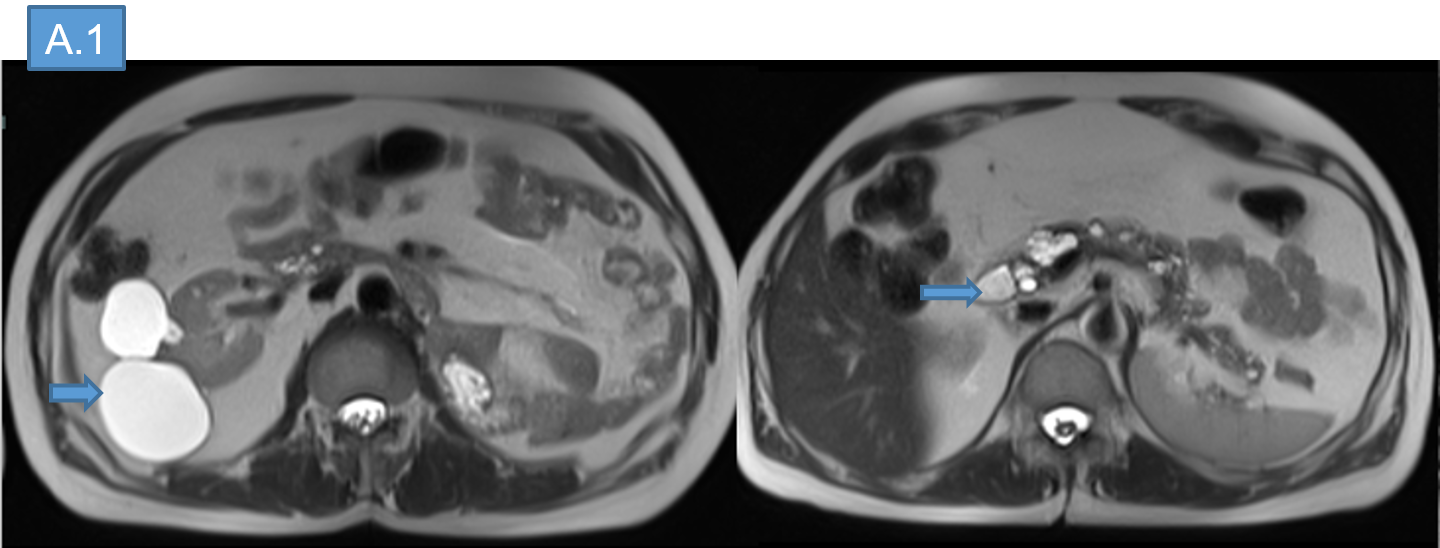
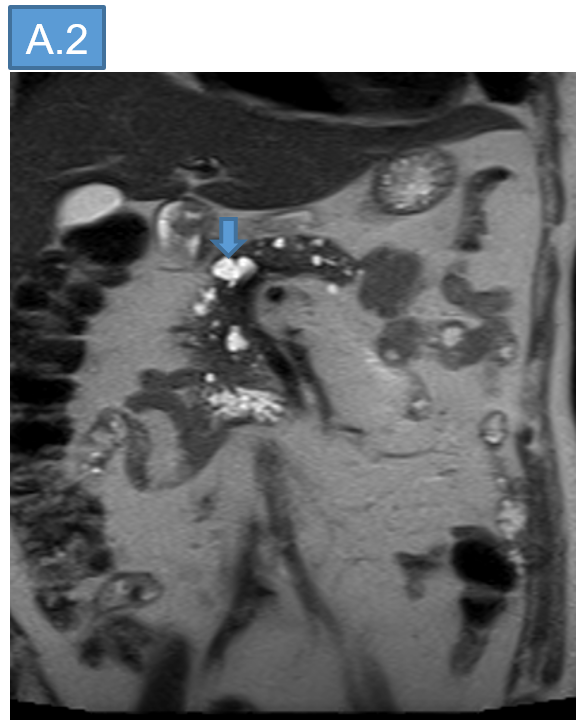
- A : MR ABDOMEN AND PELVIS.
- B : MR SPINE.

- A.
- Status post total nephrectomy on left side. No local recurrence.
- Multiple simple renal cortical cysts in right kidney.
- Multiple multilocular cystic lesions of varying sizes showing T1 hypointensity, T2 hyperintensity within the head, neck, body and tail of the pancreas.
- B.
- Long segment syringomyelia with gliosis involving the entire length of spinal cord.
- Focal T2 isointense soft tissue lesions involving the inferior aspect of medulla and intramedullary lesion at C2-C3 level with prominent flow voids.
- Multiple other nodular intramedullary foci measuring ~2-3 mm are seen at C1, C2, C4-C5 and C6 levels.
- Similarly eccentric intramedullary lesion also noted in the thoracic at T4 level.
- Few other small nodular foci in conus and along cauda equina nerve roots at L2-L3 and S2 levels.
- Anterior longitudinal ligament these lesions showed enhancement (post contrast images not provided)

DIAGNOSIS:
- Multiple simple renal cortical cysts in right kidney.
- Multiple multilocular cystic lesions of varying sizes scattered throughout the pancreas possibly cystadenomas.
- Spinal Hemangioblatomas.
Diagnosis: von Hipple Lindau syndrome.
DISCUSSION:
- Von Hippel-Lindau (VHL) disease is a rare, autosomal dominant inherited syndrome that affects the germline of the VHL gene, a tumor suppressor gene.
- VHL disease is characterized by the multisystemic development of a variety of benign and malignant tumors, especially in the central nervous system (CNS).
Mutations in the VHL tumor suppressor gene on chromosome 3p ⇒ Inactivation of the VHL protein ⇒ Increased expression of factors such as PDGF and VEGF ⇒ Angiogenesis and tumorigenesis.
The mean age at symptom onset is 33 years. Despite medical advances, the average life expectancy of patients with VHL disease is 49 years.
Haemangioblastoma:
- Well-circumscribed masses that usually abut a pial surface.
- MC - Infratentorial (dorsal half of the cerebellum, medulla)
- Supratentorial: pituitary stalk
- Intraspinal - multiple and associated with syrinx.
Retinal Hemangioblastomas ("Angiomas"):
- Typical ocular lesions of VHL
- Small, multifocal, and identical in histopathology to CNS HBs
- CT: Haemorrhagic retinal detachments - hyperdense compared with normal vitreous.
- MR: Tiny enhancing nodules on T1 C+
Other manifestations:
- Endolymphatic Sac Tumors: Slow-growing, benign but locally aggressive papillary cyst adenomatous tumors of the endolymphatic sac. Grossly - vascular heaped up tumors along petrous temporal bone.
- Phaechromocytomas
- Pancreatic cysts
- Multiple simple renal cysts as well as multiple mixed solid and cystic renal neoplasms.
Management:
- Most lesions from VHL are treatable and surveillance is recommended with various regional guidelines.
- Some experts advocate routine screening starting in adolescence.
- Prognosis is poor, with a median survival of ~50 years, with the most common cause of death being renal cell carcinoma and cerebellar haemangioblastoma.
Follow-up evaluations recommended for patients with VHL disease:
- Annual screening (ophthalmoscopy, physical/neurologic examination) beginning in infancy or early childhood.
- Brain MRs - every 1-3 years starting in adolescence.
- Annual abdominal MR or ultrasound screening for RCC and pancreatic tumors is recommended annually, beginning at age 16.
- Blood pressure should be monitored and 24-hour urine catecholamine's obtained annually.
REFERENCES:
Imaging manifestations of von Hippel-Lindau disease: an illustrated guide focusing on the central nervous system:
- 2022 May-Jun;55(3):188–192. doi: 10?1590/0100-3984?2021?0080-en
- Radio Graphics 2018; 38:849–866
https://doi.org/10.1148/rg.2018170156
Dr ANITA NAGADI
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr NEHA SATHYANARAYANA
Radiology Resident
Manipal Hospital, Yeshwanthpur, Bengaluru.

