
A 51 year old male presenting with giddiness, headache, vomiting and neck pain with right upper limb pain. On examination, right upper limb was pale and cold; absent right radial artery pulsation.
A 51-year-old male presented with giddiness, headache, vomiting and neck pain with right upper limb pain. On examination, right upper limb was pale and cold; absent right radial artery pulsation.
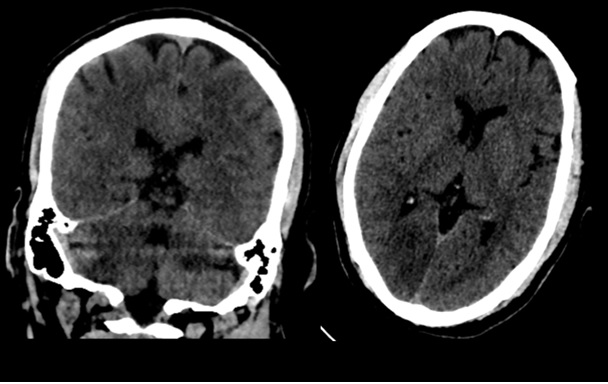
- Image 1: NCCT; Ill-defined hypodense area with loss of grey-white matter differentiation in right cerebellar hemisphere and right occipital lobe in keeping with acute infarcts in the right PCA territory.
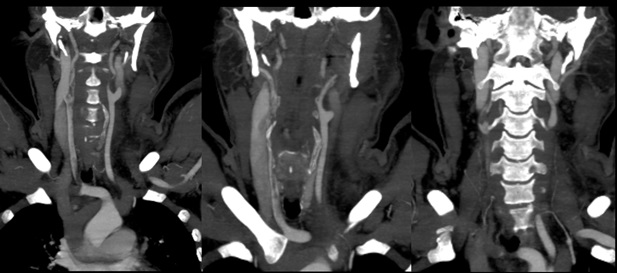
- Image 2: CT angiography of head and neck shows absent contrast opacification in the right subclavian artery, eccentric filling defect in right CCA, carotid bulb and ICA.
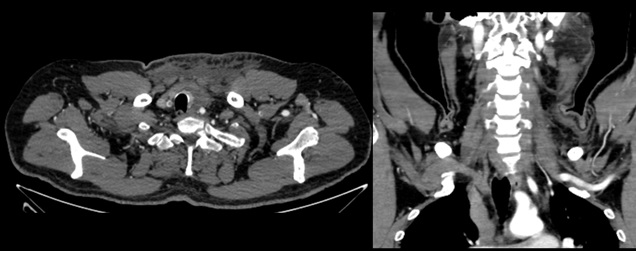
- Image 3: Ovoid lesion in continuity with right subclavian artery in keeping with completely thrombosed aneurysm in third part right subclavian artery.
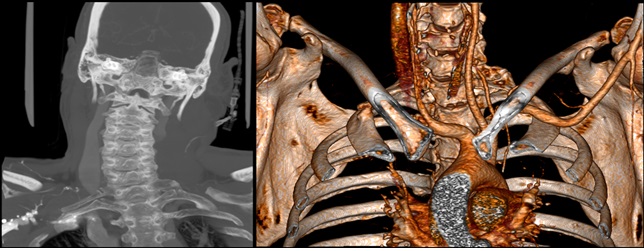
- Image 4: Coronal MIP and VR images show right complete cervical rib (type 1) with complete bony fusion of the cervical rib (red and turquoise arrow) with the right first thoracic rib (yellow arrow). Incomplete left cervical rib with distal fibrous band attachment (type 3) (green arrow).
- Image 5: Intra-op and post-op images show clots removed from the thrombosed artery and aneurysm.

DIAGNOSIS AND DISCUSSION:
- Right PCA territory infarct with thrombosis of the right brachiocephalic artery, right CCA, ICA; thrombosed aneurysm in right subclavian artery, secondary to right cervical rib.
Discussion:
- The cervical rib aka neck rib or supernumerary rib is a congenital overdevelopment of the transverse process of a cervical spine vertebra.
- These occur in approximately 0.5 to 1% of the population.
- Most cervical ribs go unnoticed throughout life and are clinically irrelevant.
- However, in some cases, they can cause localized pain and compress surrounding structures, leading to intervention.
- It can cause thoracic outlet syndrome from compression of artery/vein/nerve.
- Arterial thoracic outlet syndrome is a rare condition characterized by a subclavian artery pathology associated with a bone abnormality. It is rarely associated with thromboembolic stroke.
REFERENCES:
- https://www.ncbi.nlm.nih.gov/books/NBK541001/#:~:text=A%20cervical%20rib%2C%20also%20known,to%201%25%20of%20the%20population.
- Celier A, Chabay S, Maurizot A, Cochennec F, Stanciu D, Pico F. Posterior cerebral artery stroke by reverse flow embolism in thoracic outlet syndrome – a case report. BMC Neurol. 2020 Jun 4;20(1):229. doi 10.1186/s12883-020-01797-y. PMID: 32498705; PMCID: PMC7271554.
- Owen P. Palmer, Fred A. Weaver. Bilateral Cervical Ribs Causing Cerebellar Stroke and Arterial Thoracic Outlet Syndrome: A Case Report and Review of the Literature. Annals of Vascular Surgery, Volume 29, Issue 4, 2015, Pages 840.e1-840.e4, ISSN 0890-5096, https://doi.org/10.1016/j.avsg.2014.12.008.
We would like to thank, Dr Krishna Chaitanya (Consultant vascular surgeon) and Dr Mayank Kumar Srivastava (Junior consultant neurologist) for their contributions.
Dr. Vikas H P
Radiology Resident,
Columbia Asia Radiology Group
Dr. Anita Nagadi
MD, MRCPCH (UK), FRCR (UK), CCT (UK)
Senior Consultant Radiologist
Columbia Asia Radiology Group.
