
A 45 year old male with complaints of pain and sudden loss of vision in left eye.
- A 45 year old male with complaints of pain and sudden loss of vision in left eye.
- On examination the extraocular movements were restricted in all directions. Pupil mid dilated and fixed. Left III, IV,V1 nerve palsy.
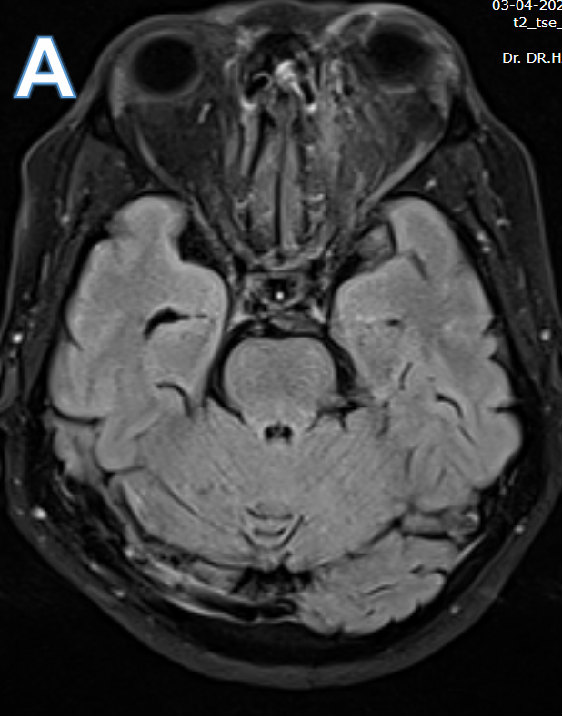
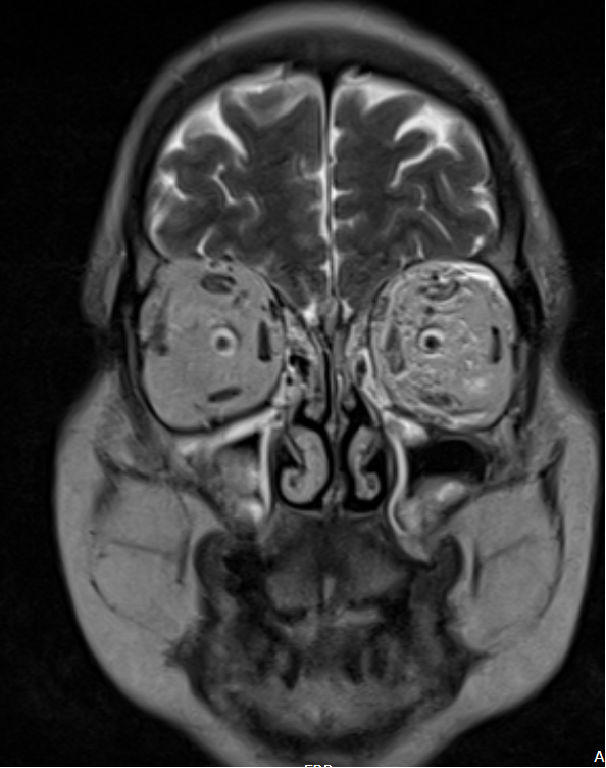

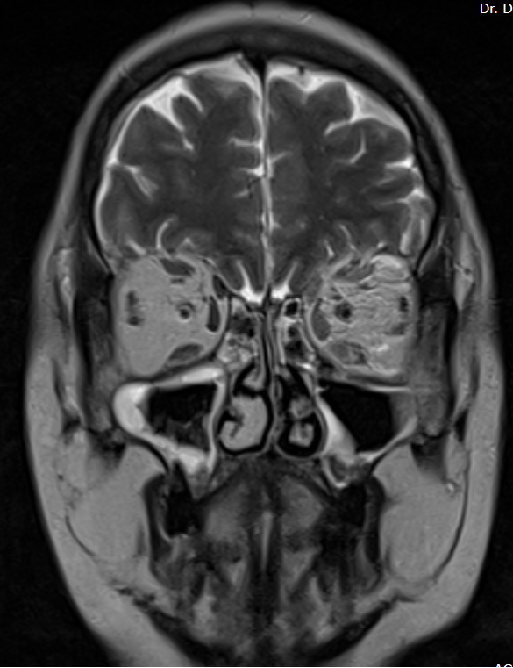


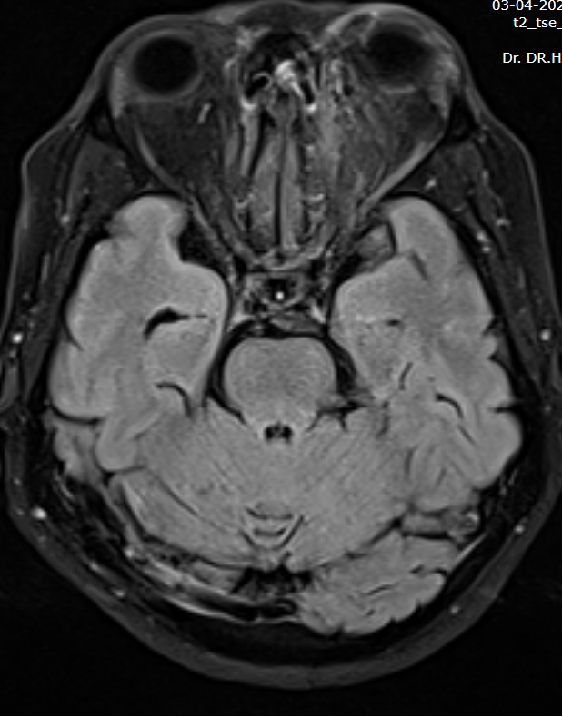
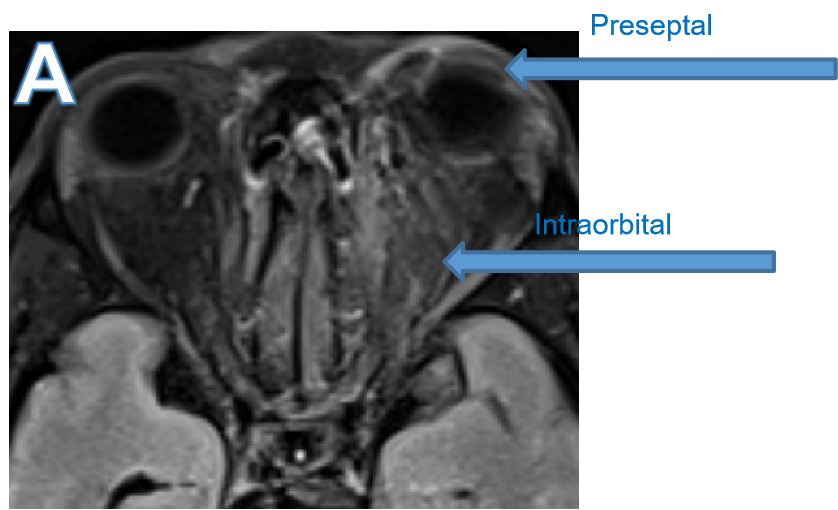
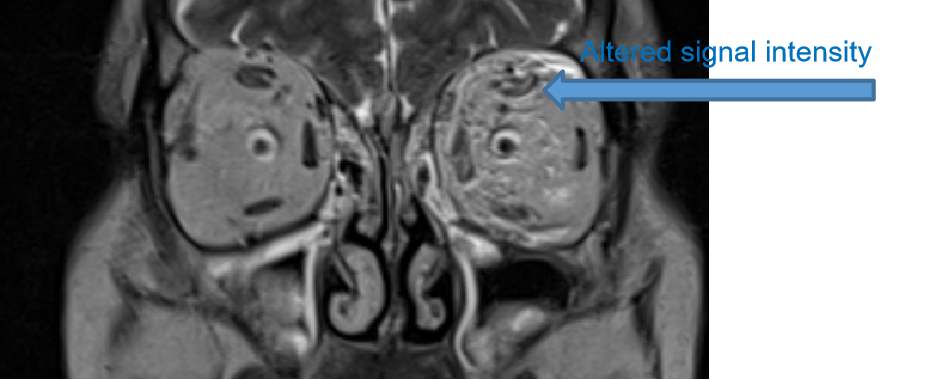
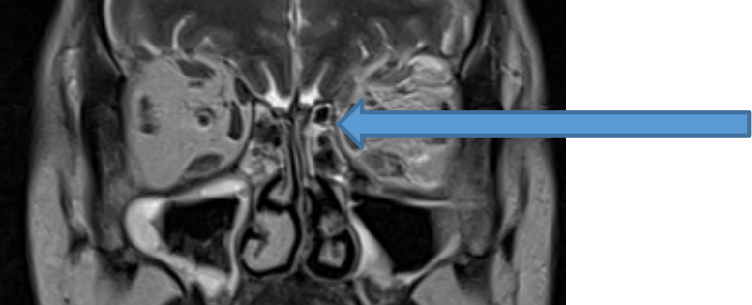
- A. Diffuse T2 FLAIR hyperintensity involving the left intraorbital fat and preseptal soft tissue with mild restricted diffusion. Mildly bulky and altered signal intensity involving the left extraocular muscles.
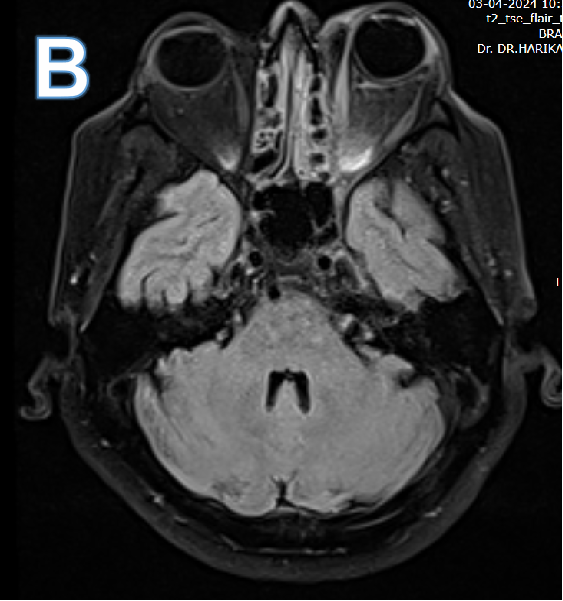
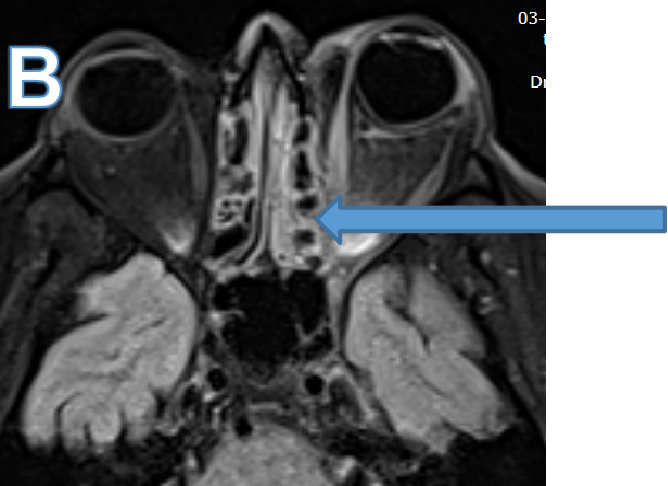
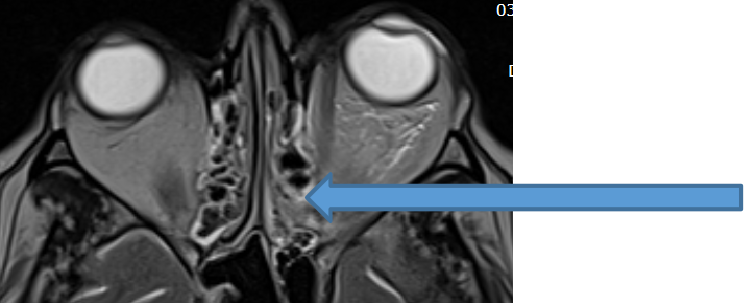
- B. Adjacent left ethmoid air cells demonstrate T2/FLAIR hyperintensity suspicious for contiguous infective intraorbital spread of sinus disease.
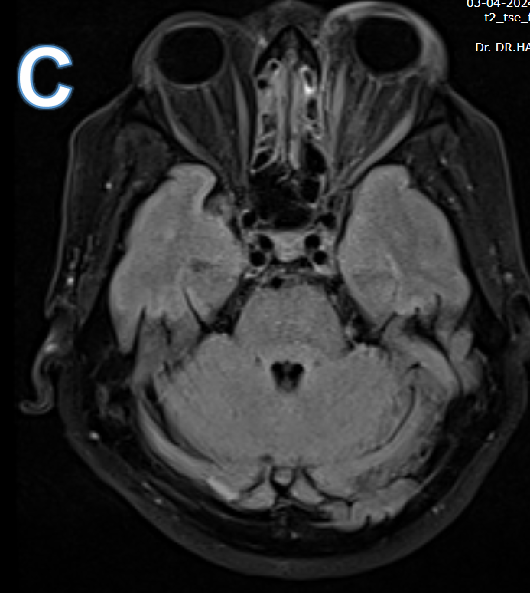
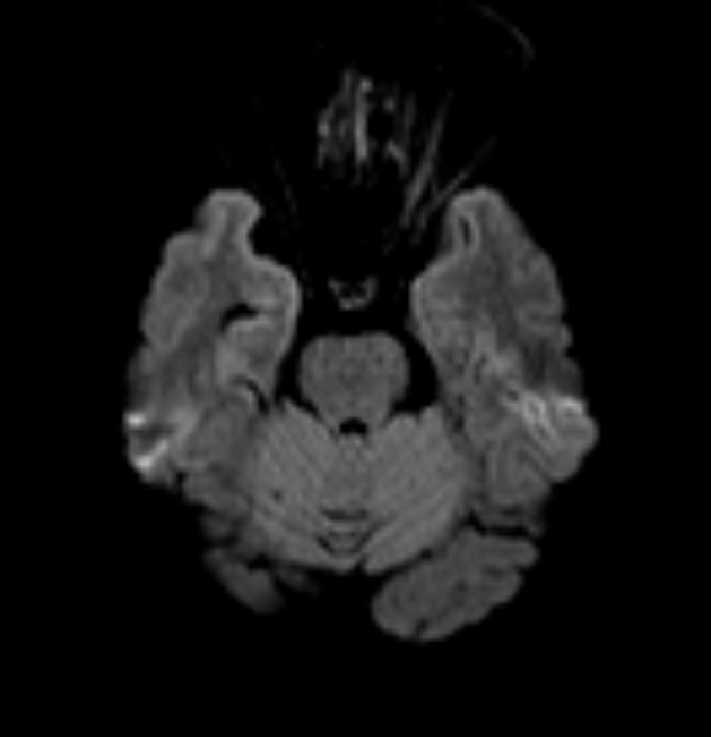
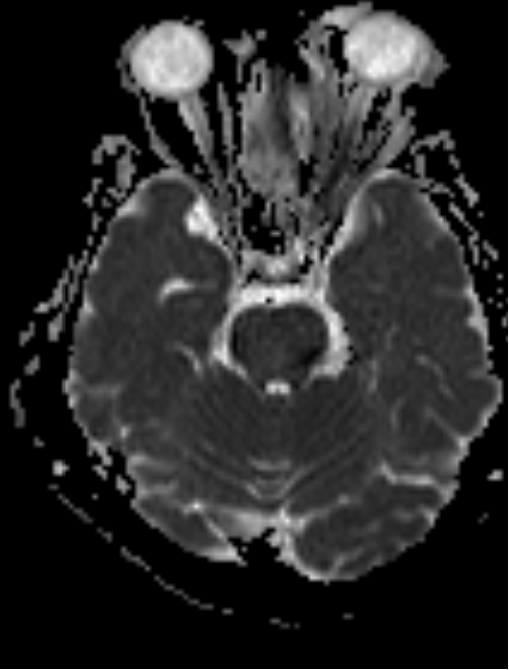
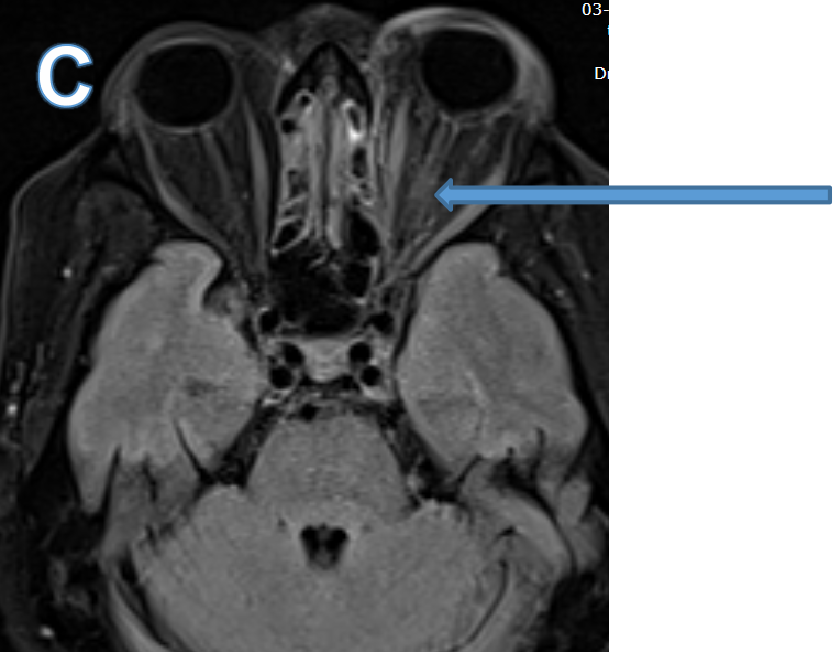
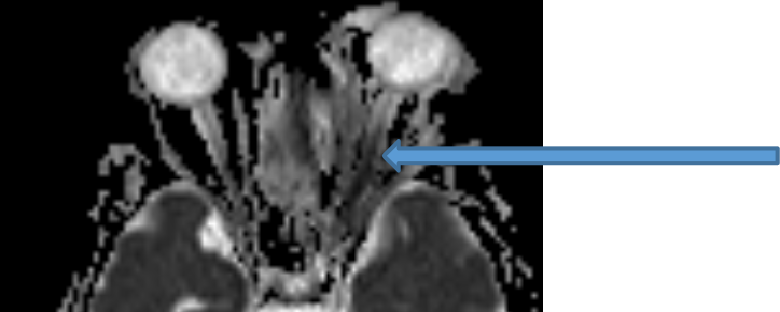
- C. Mild T2 FLAIR hyperintensity with restricted diffusion involving the intraorbital and intracanalicular segment of the left optic nerve representing ischemic optic neuritis.
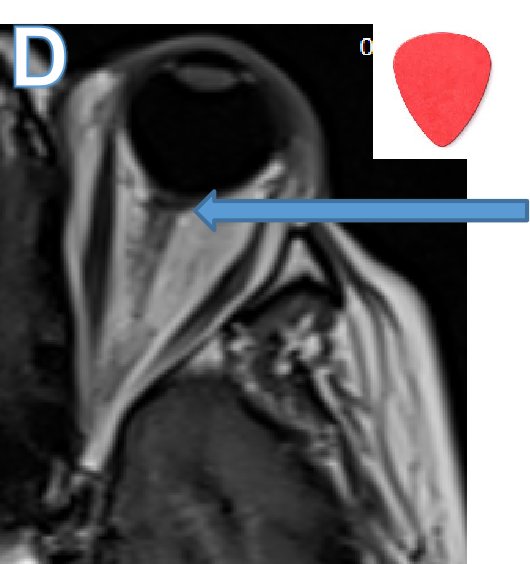
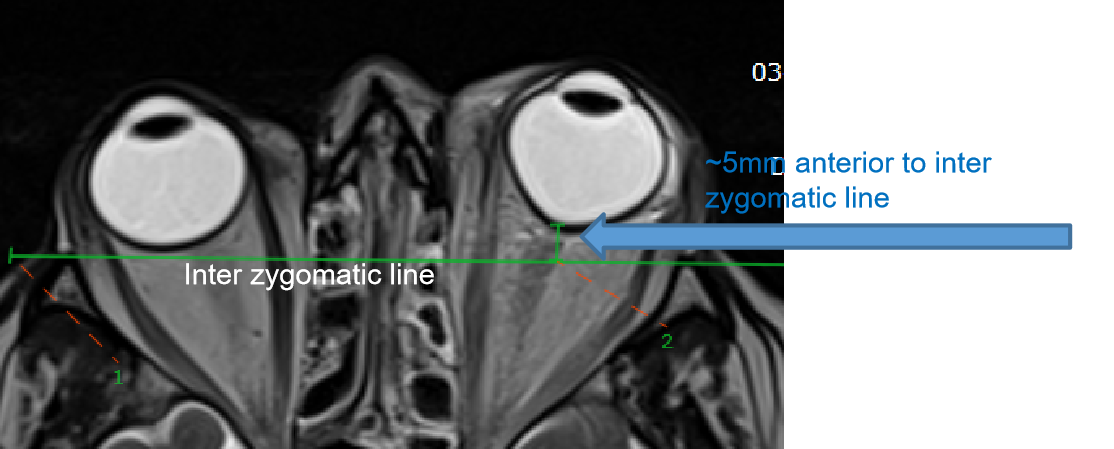
- D. The posterior surface of the left orbital globe demonstrates mild coning / tenting at the optic nerve insertion with a guitar pick sign morphology.

DIAGNOSIS:
- Diffuse left intraorbital and preseptal fat stranding with bulky, altered signal intensity of the left extraocular muscles.
- Ischemic left optic neuritis.
- Left sided proptosis with mild tenting of the posterior scleral surface of the left orbital globe indicating increased orbital pressure.
Diagnosis - Left orbital cellulitis with orbital compartment syndrome and ischaemic optic neuritis
DISCUSSION:
- Orbital cellulitis is one of the most common orbital pathologies. It is primarily diagnosed clinically and confirmed by imaging modalities such as CT or MRI.
- MRI is better because of its increased slice orientation , superior anatomic (T1-weighted) and pathologic (T2-weighted [T2W]) resolution. MRI provides excellent contrast resolution in the orbit. Useful for demonstrating intracranial extension.
- T1-W contrast-enhanced imaging with fat suppression is the gold standard in the detection and characterization of orbital pathology, T2W FS have similar sensitivity.
- Type - preseptal (periorbital) or postseptal (orbital).
- Causes - Paranasal sinusitis (MC), middle ear, or face infections, trauma , foreign body, ophthalmic surgery, peribulbar anaesthesia, infected mucocele eroding orbit, immunodeficiency.
- It causes diffuse, oedematous infiltration of the orbital connective tissue, swelling and ill-defined margins of the extraocular muscles and exophthalmos .
- Complication - Orbital/periorbital abscess, optic neuritis/perineuritis, intracranial involvement , dacryoadenitis, cavernous sinus thrombophlebitis, subdural/epidural empyema. mycotic aneurysm of the internal carotid artery, cerebritis, brain abscess, and meningitis.
- Treatment - Uncomplicated orbital cellulitis with antibiotics. Surgery is indicated in patients with intracranial extension, poor or failure to respond to antibiotic therapy, worsening visual acuity or pupillary changes, or evidence of an abscess.
Orbital compartment syndrome
- Ophthalmological emergency.
- Causes - Acute orbital haemorrhage due to trauma, surgery, fulminant orbital cellulitis, intraorbital abscess, orbital emphysema, tumours.
- Sequelae - central retinal artery occlusion, direct compressive optic neuropathy, ischemic optic neuropathy.
- Treatment - Lateral canthotomy and inferior cantholysis. In unresponsive cases incision of the orbital septum and orbital bony decompression may be necessary.
REFERENCES
- Jyani R, Ranade D, Joshi P. Spectrum of Orbital Cellulitis on Magnetic Resonance Imaging. Cureus. 2020 Aug 11;12(8):e9663. doi: 10.7759/cureus.9663. PMID: 32923259; PMCID: PMC7485920.
- Vanessa Lima, Benjamin Burt, Igal Leibovitch, Venkatesh Prabhakaran, Robert A. Goldberg, Dinesh Selva,Orbital Compartment Syndrome: The Ophthalmic Surgical Emergency,Survey of Ophthalmology,2009,ISSN 0039-6257.
- Danishyar A, Sergent SR. Orbital Cellulitis. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
Dr HARSHA CHADAGA
Senior Consultant Radiologist
Head of the Radiology
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr SHIKHA JOSHI
Radiology Resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
