
A 40-year old female with pregnancy of five months duration and suspicion of a pelvic mass and per vaginal bleeding since 1 week.
A 40-year old female with pregnancy of five months duration and suspicion of a pelvic mass and per vaginal bleeding since 1 week.
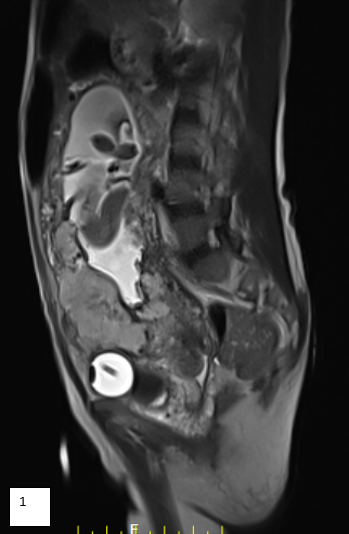

- Shows a complete placenta previa (orange arrow). It is invading anterior myometrium with focal complete loss of discernible bladder wall (blue arrow).
- There is grossly increased myometrial and pelvic vascularity (orange arrow) with a T2 hypointense intraplacental band (blue arrow) (Fig 1).
- There is presence of multiple enlarged retroperitoneal collaterals (arrows) even draining into upper inferior vena cava. (Fig 3).
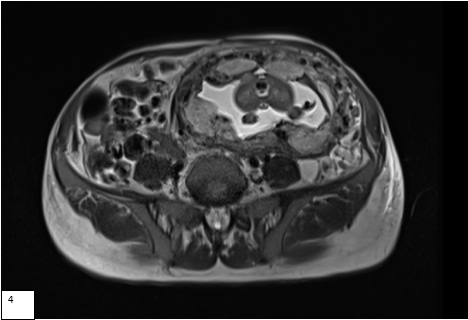
- Two lobes of placental tissue (asterix) noted on anterior and posterior myometrium connected via a vascular channel (orange arrow((Fig 4).
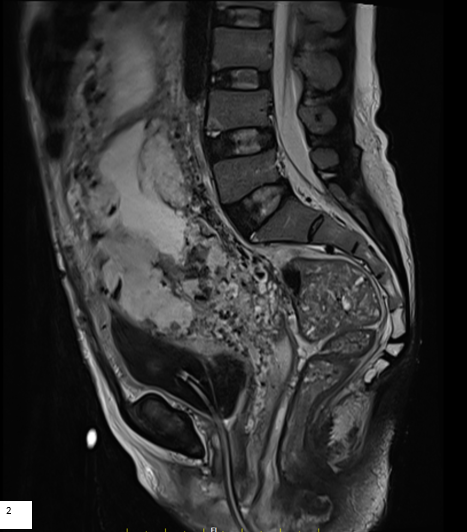
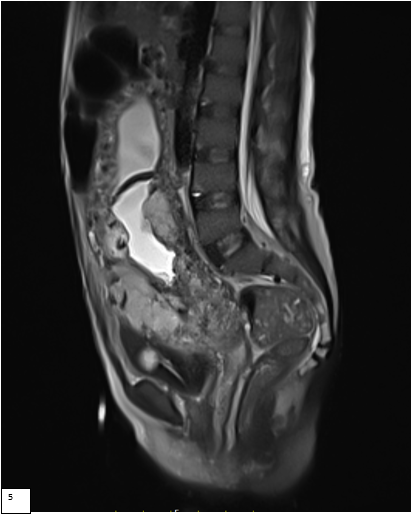
- Placental edges appear rounded with lumpy uneven placental contour. (Fig 5).
Diagnosis:
Anterior and posterior Placenta percreta and Grade IV placenta previa in a patient with bilobar placental configuration.
Discussion:
- Increasing number of caesarean sections have led to increase in frequency of placenta previa and accreta in the recent years. Accurate preoperative detection is important to reduce feto-maternal morbidity and mortality.
- Ultrasound remains the initial diagnostic tool. Low lying placenta, loss of retroplacental clear zone, multiple lacunae, rounded placental edges are indicators which should raise suspicion. An irregular bladder wall may be noted with placenta percreta.
- MRI shows lumpy placental contour with loss of uniformity of placental thickness, tethering, rounded edges, uterine bulging & placenta previa. Additional features identified with MRI include heterogenous parenchymal signal intensity and presence of dark T2 hypointense intraplacental bands.
- MRI can also accurately depict invasion into adjacent organs and increased pelvic vascularity with its drainage, as in our case; all important for presurgical planning.
- Imaging is recommended at 24- 30 weeks to allow for relative placental maturity and appearance. Imaging prior to this may not be conclusive. Imaging after 30 weeks may again confound appearance as normal ageing placenta will also show heterogenosity and presence of myometrial thinning may resemble partial invasion.
- This is a unique case in that the patient has three placental abnormalities with a Grade IV placenta previa, anterior and posterior placenta percreta and bilobar placental configuration.
- The gold standard management of placenta percreta with bladder invasion include: Cesarean hysterectomy.
REFERENCES:
- MRI of Placenta Accreta, Placenta Increta, and Placenta Percreta: Pearls and Pitfalls. AJR 2017; 208:214–221
- Magnetic resonance imaging of placenta accreta. M. Ben Ammar , A. Ben Miled, S. Zaouali, N. Zouari, A. Gaja, N. Mnif; Tunis/TN. ECR 2016 / C-1463
Dr. Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Manipal Hospitals Radiology Group.
Dr. Sushant Mittal
MD, Cross-sectional fellow
Manipal Hospitals Radiology Group.

