A 4-year-old child with complaints of right eye swelling ,restricted ocular motility and diminished vision since 10 days
A 4-year-old child with complaints of right eye swelling ,restricted ocular motility and diminished vision since 10 days.
- A 4 year old child with complaints of right eye swelling ,restricted ocular motility and diminished vision.
- The patient had occasional history of consumption of meat from food vendors.
FINDINGS:
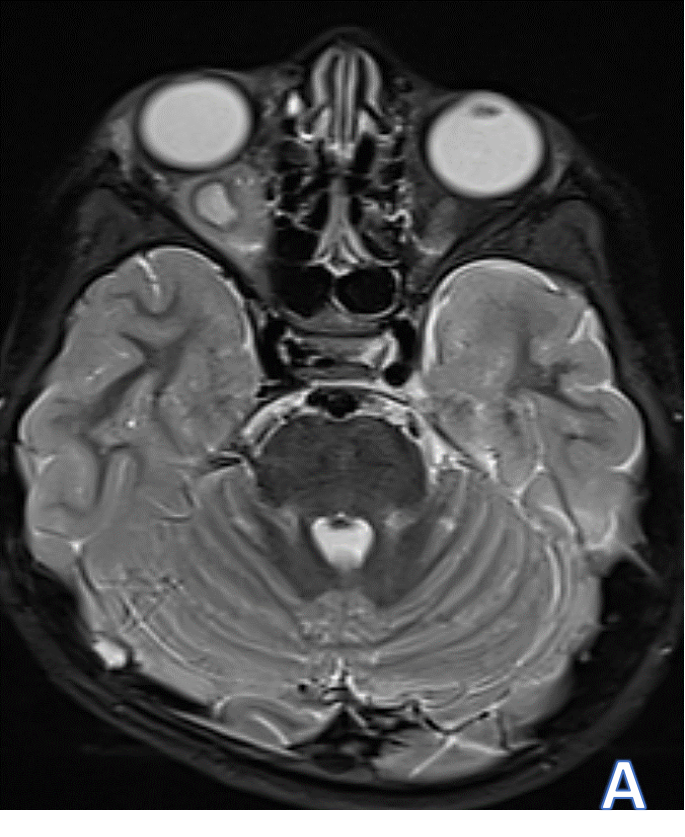
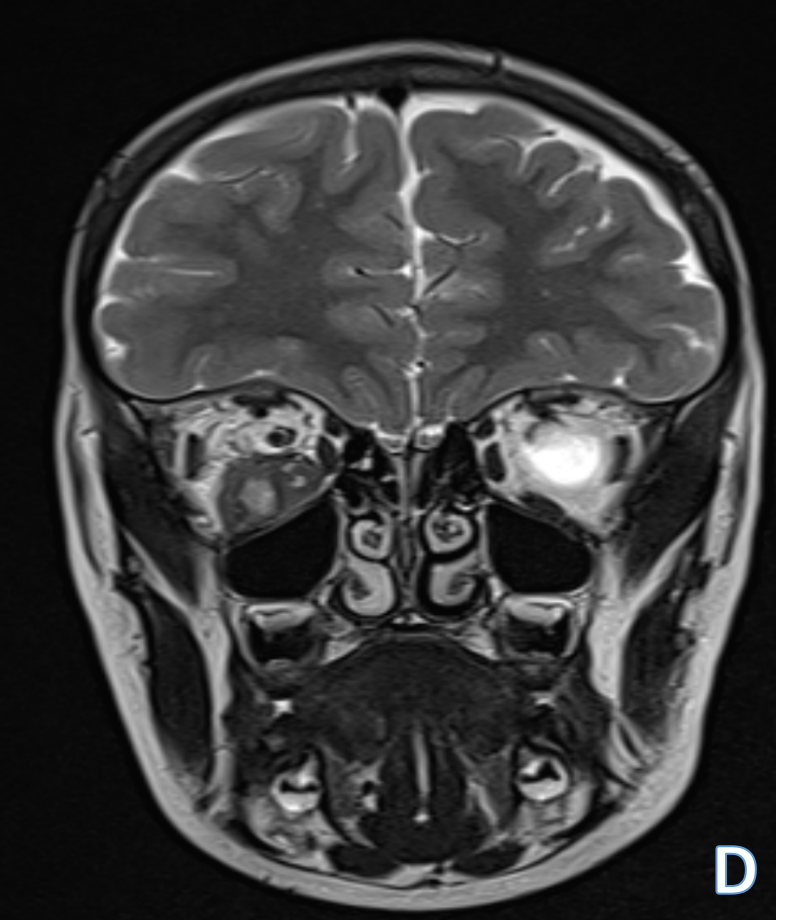
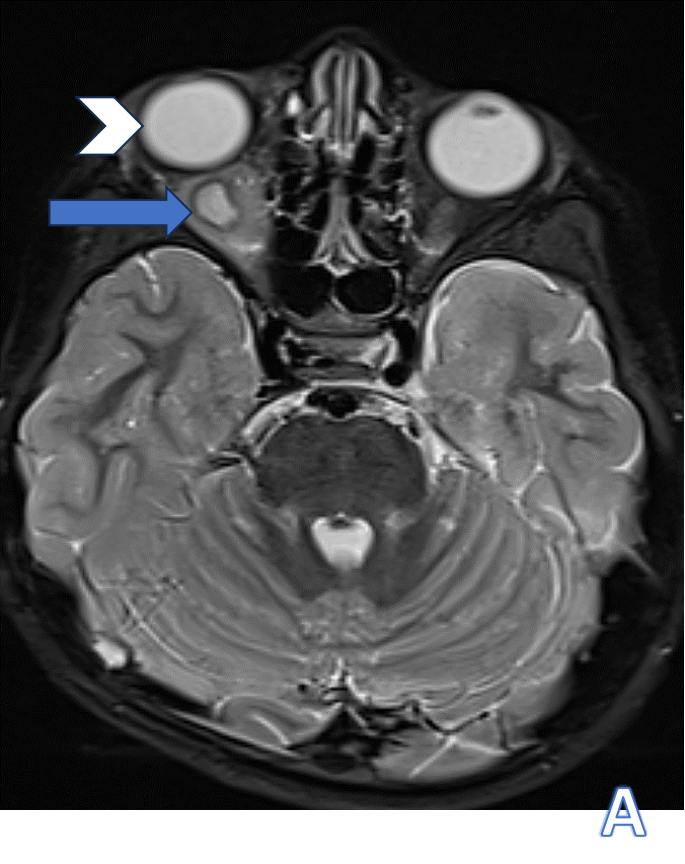
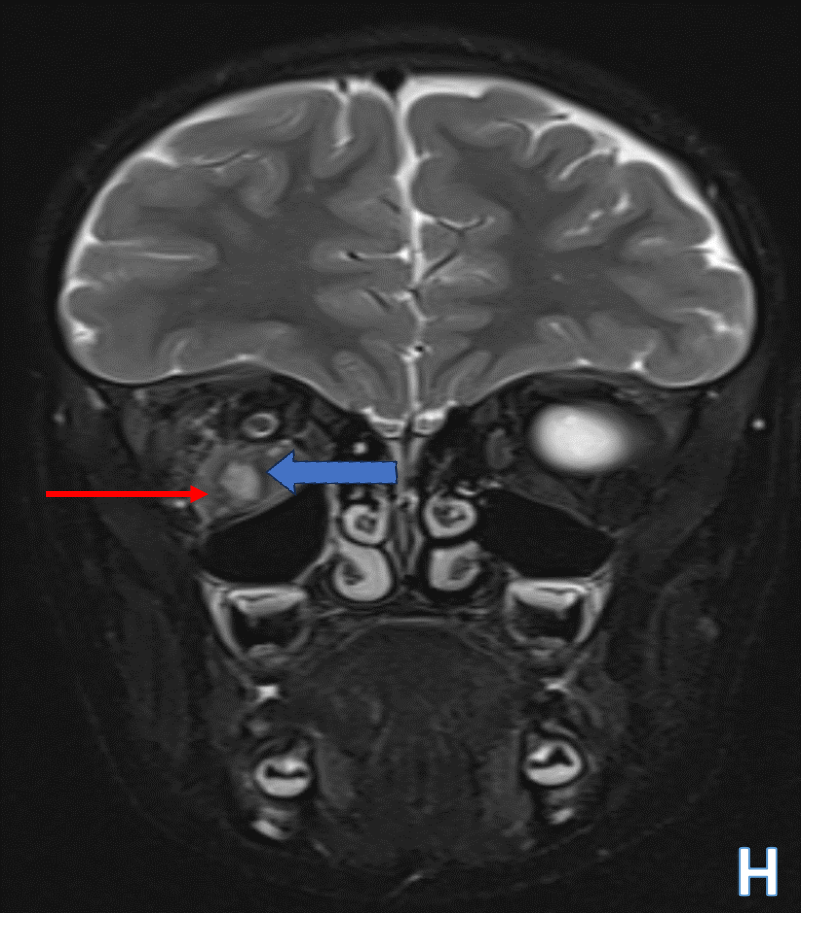
- Mild proptosis of right globe(white arrowhead in figure A)
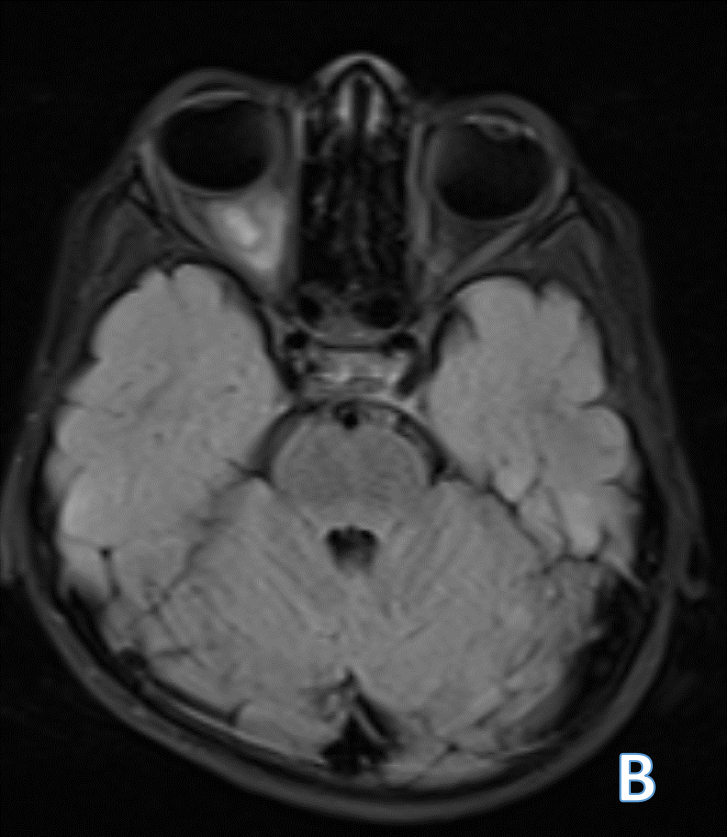
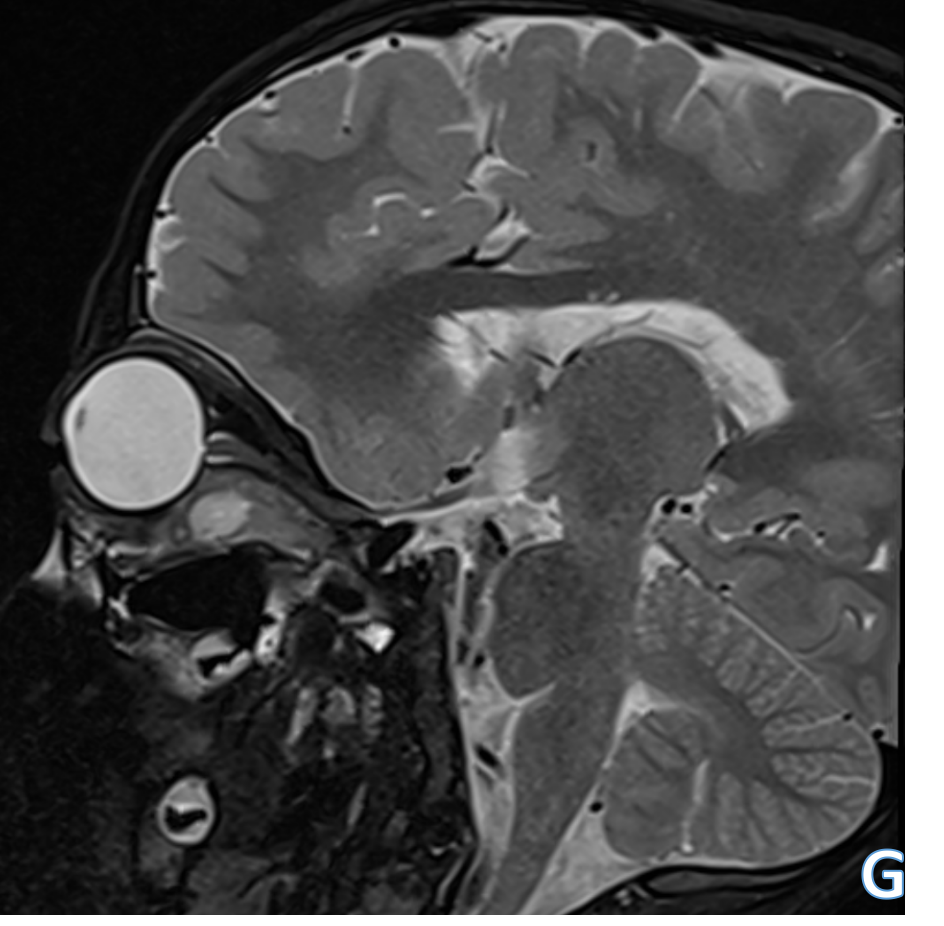
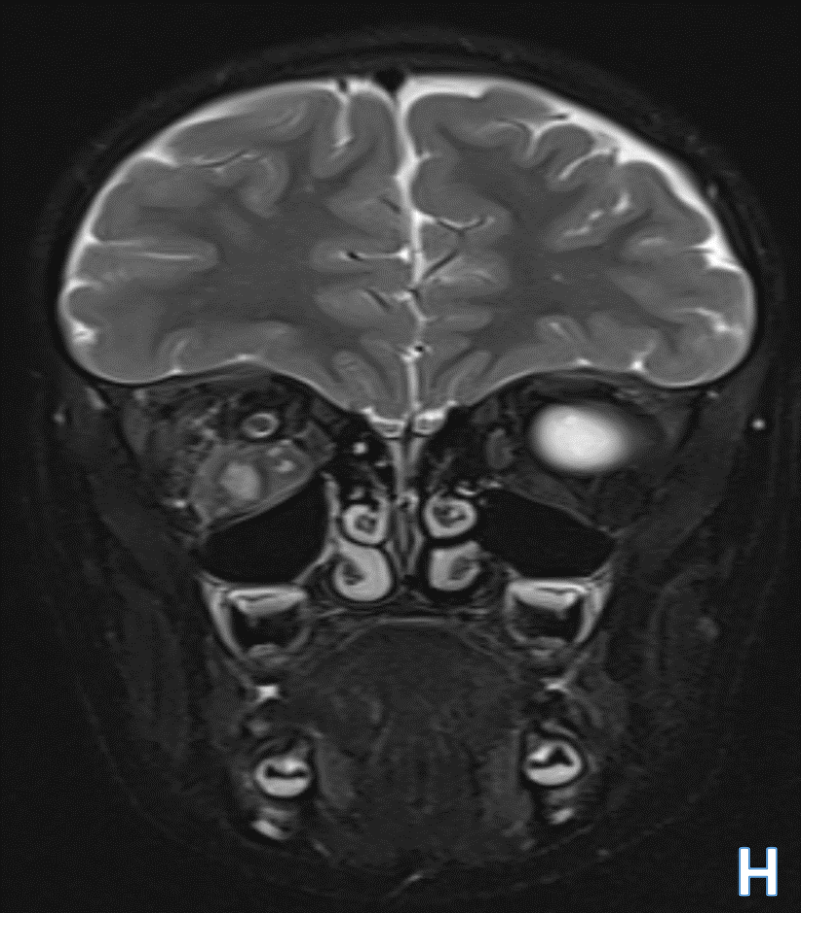
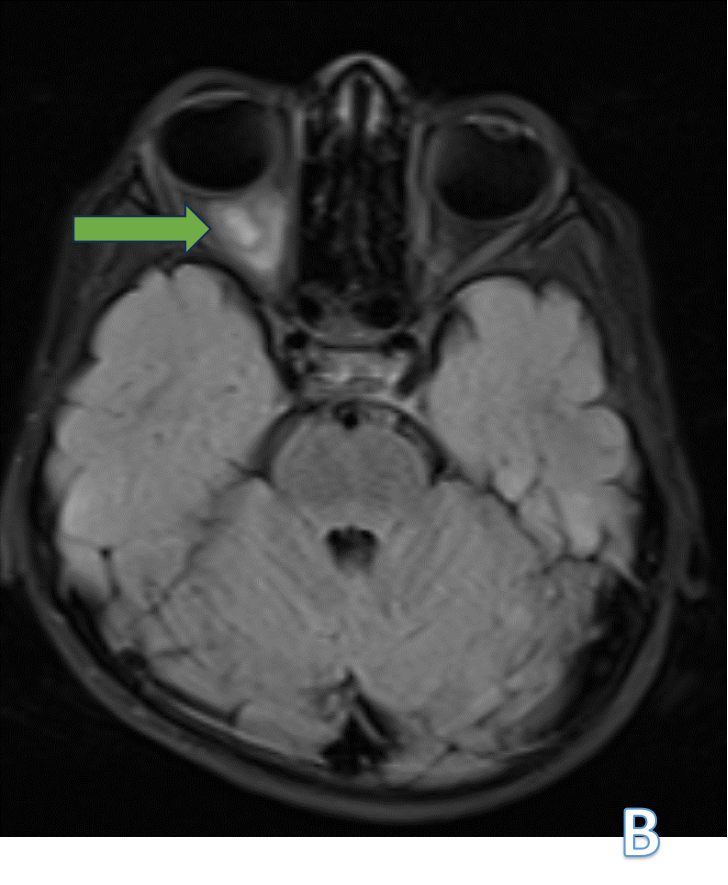
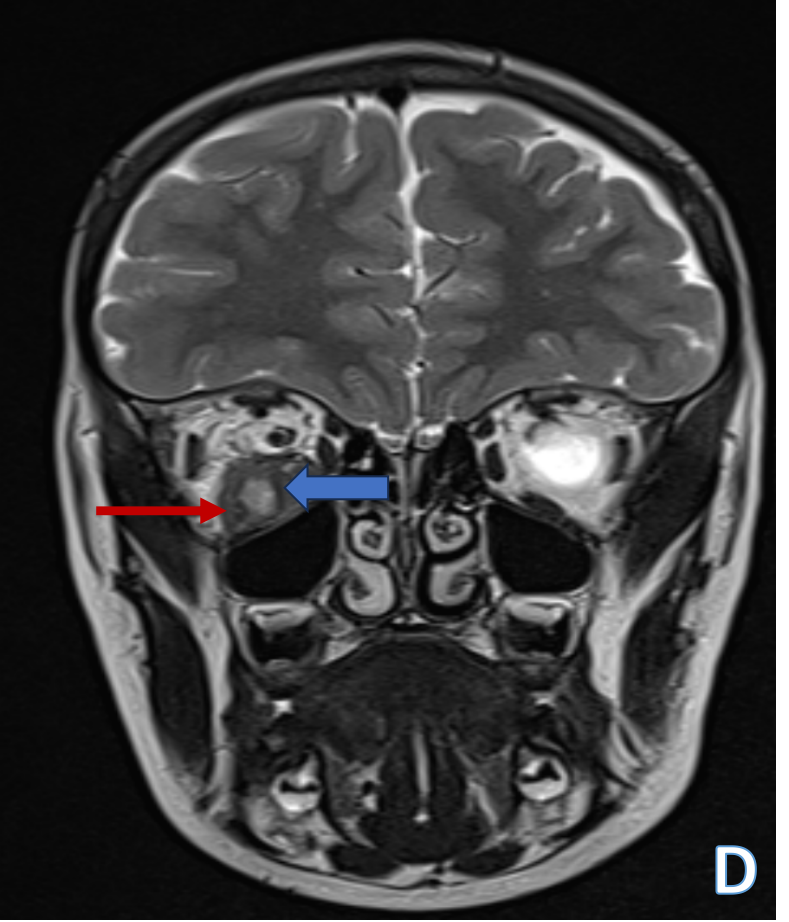
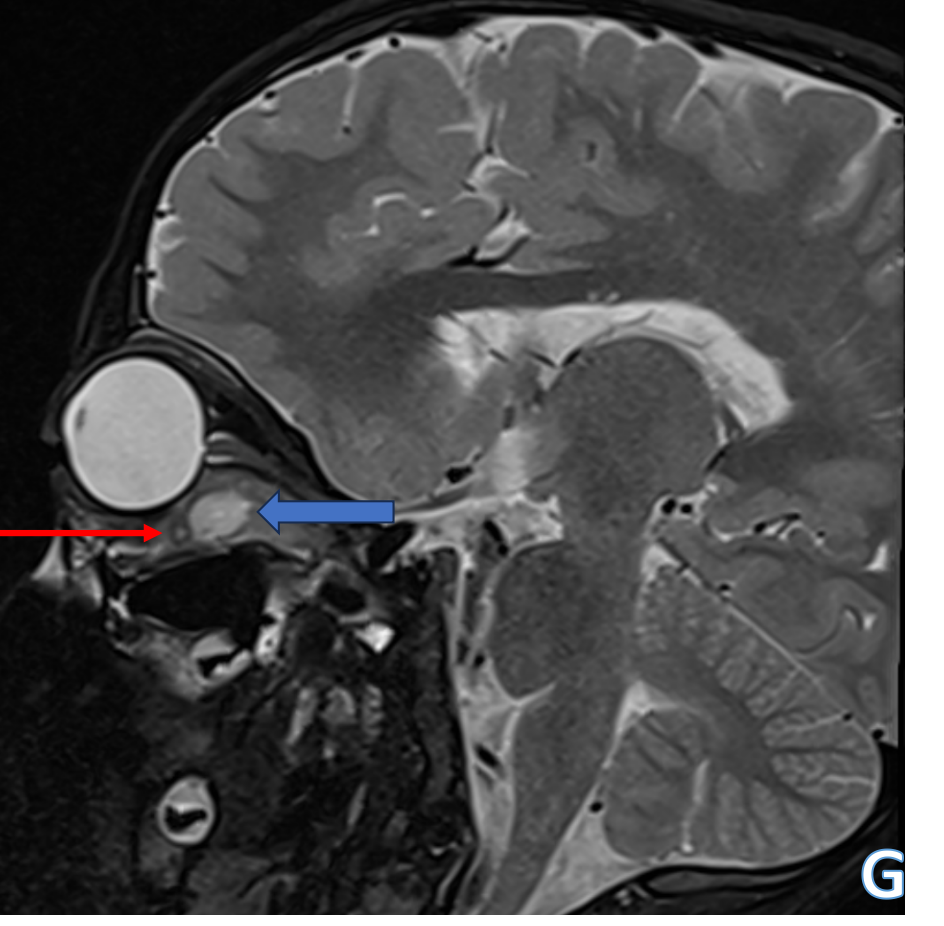
- The right inferior rectus muscle is bulky and edematous with a well defined cystic lesion within the muscle showing T2 hyperintensity(blue arrows in figure A,D,G&H) with incomplete FLAIR suppression(green arrow in figure B).
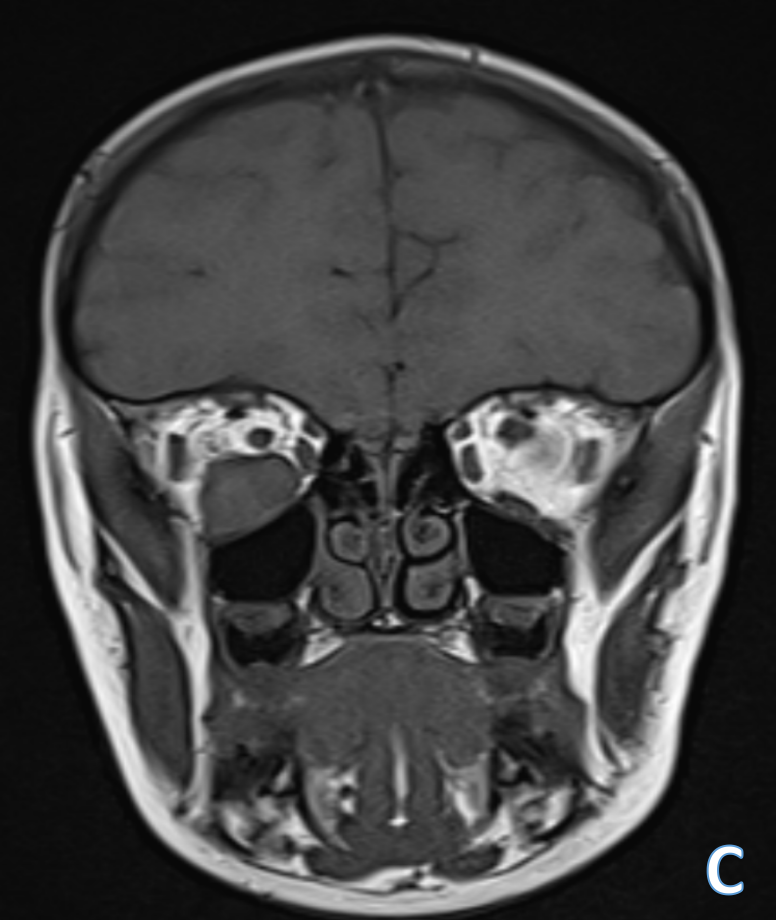
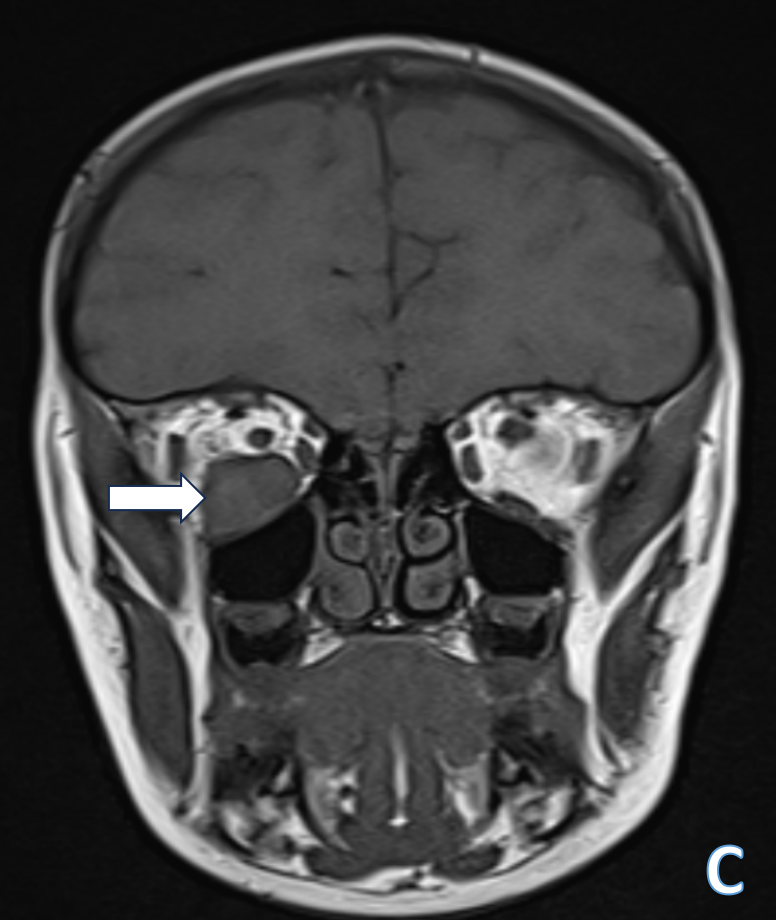
- The lesion shows T1 isointense signal(white arrow in figure C) indicating no internal fat or hemorrhagic component
- A small eccentric speck of hypointensity seen within the lesion in anterior aspect(red arrows in figures D, G&H)- indicative of scolex
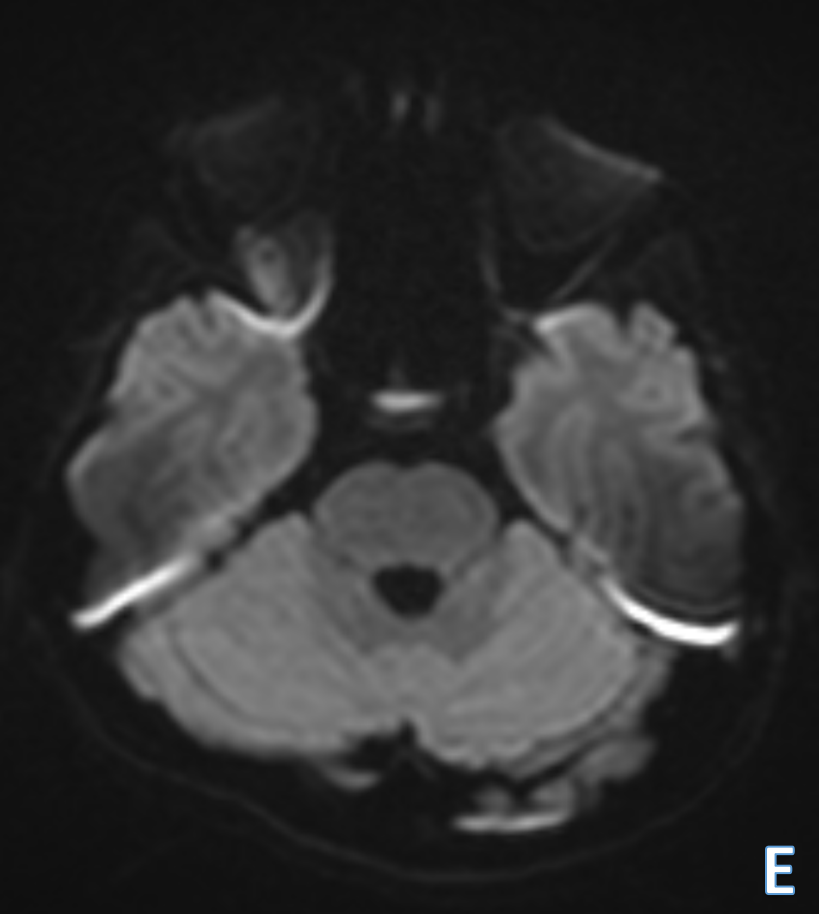
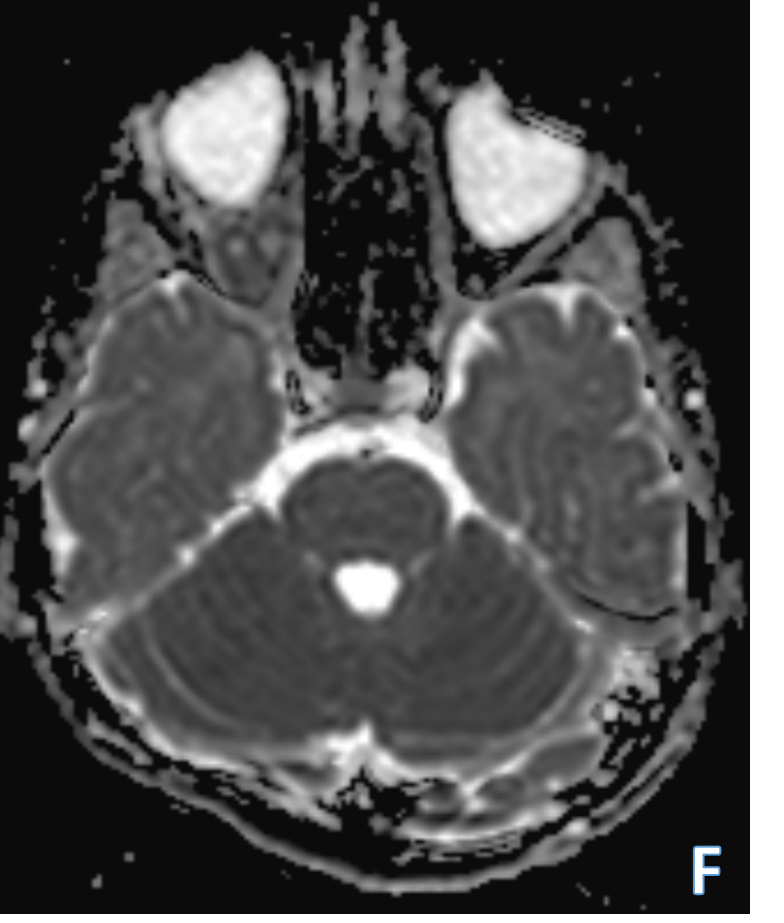
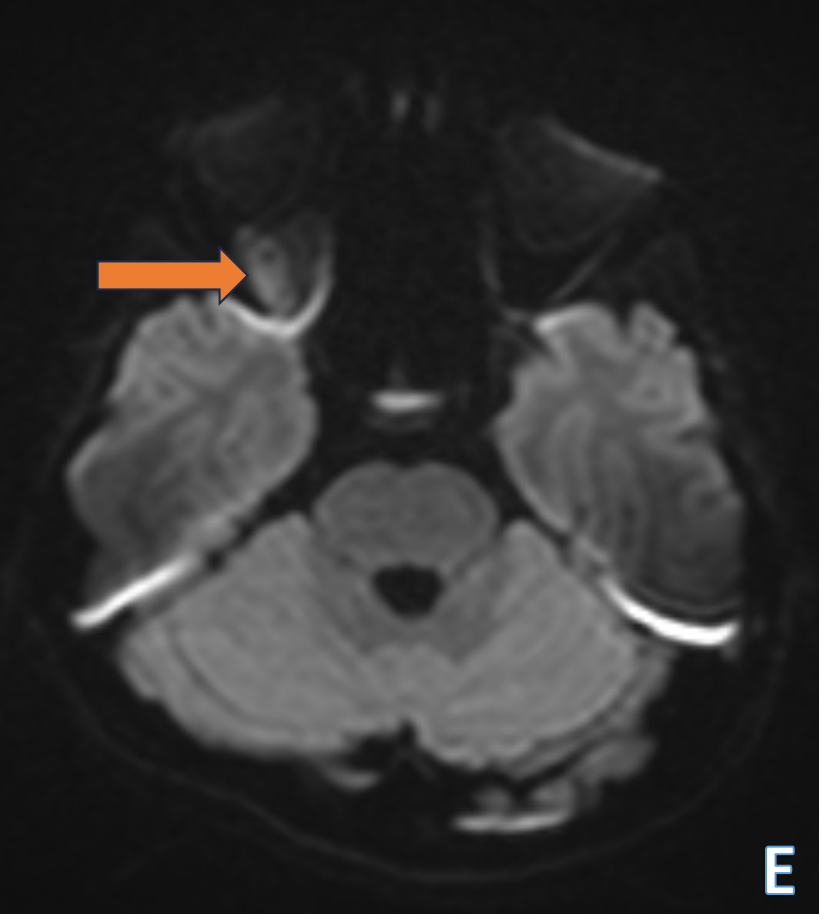
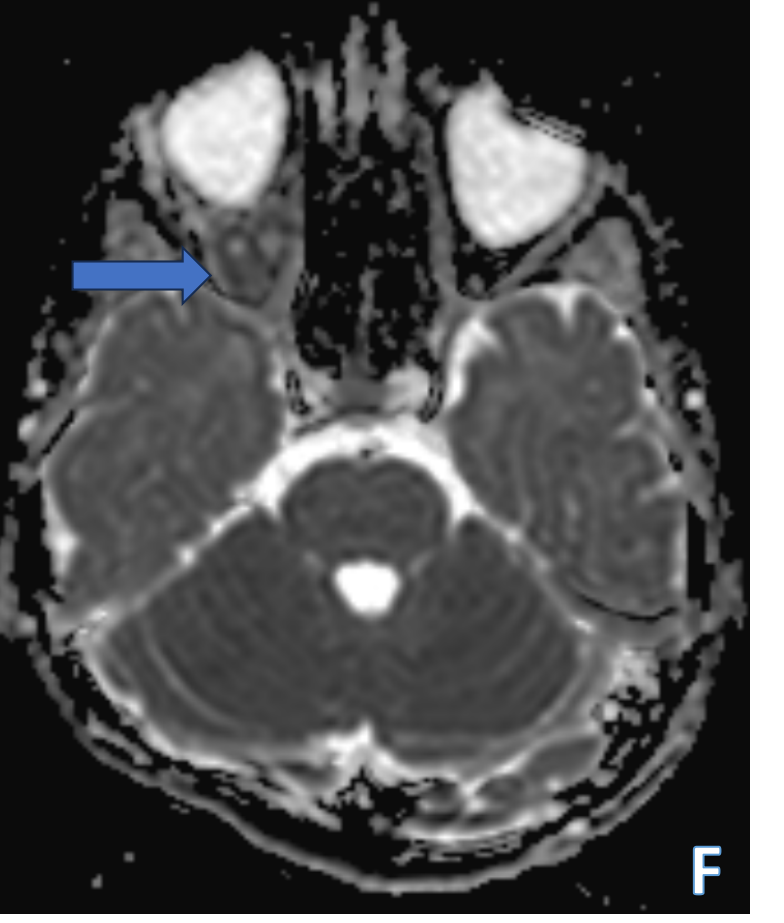
- The lesion shows restriction on DWI( orange and blue arrows in figures E&F respectively)
- Rest of the intraorbital muscles are normal.
DIAGNOSIS:
- ORBITAL CYSTICERCOSIS
DISCUSSION:
- Cysticercosis is a preventable and eradicable cause of blindness endemic in the Indian subcontinent, South-East Asia and other developing countries.
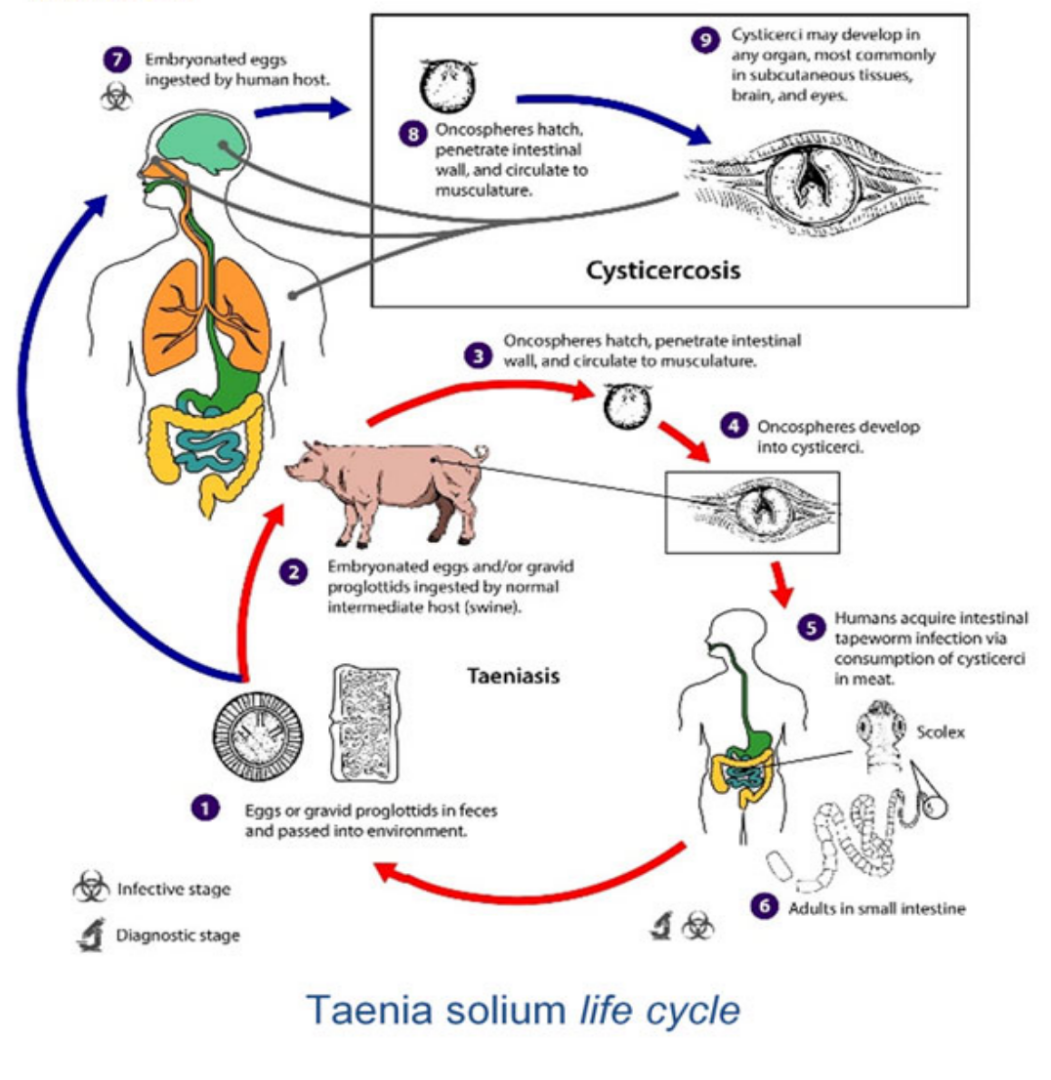
- It is a parasitic infestation caused by Cysticercus cellulosae, the larval form of Taenia solium.
- The target organs usually involved are the brain, eyes, spine, and skeletal muscles.
- The occurrence of ocular cysticercosis with no other systemic involvement is rare
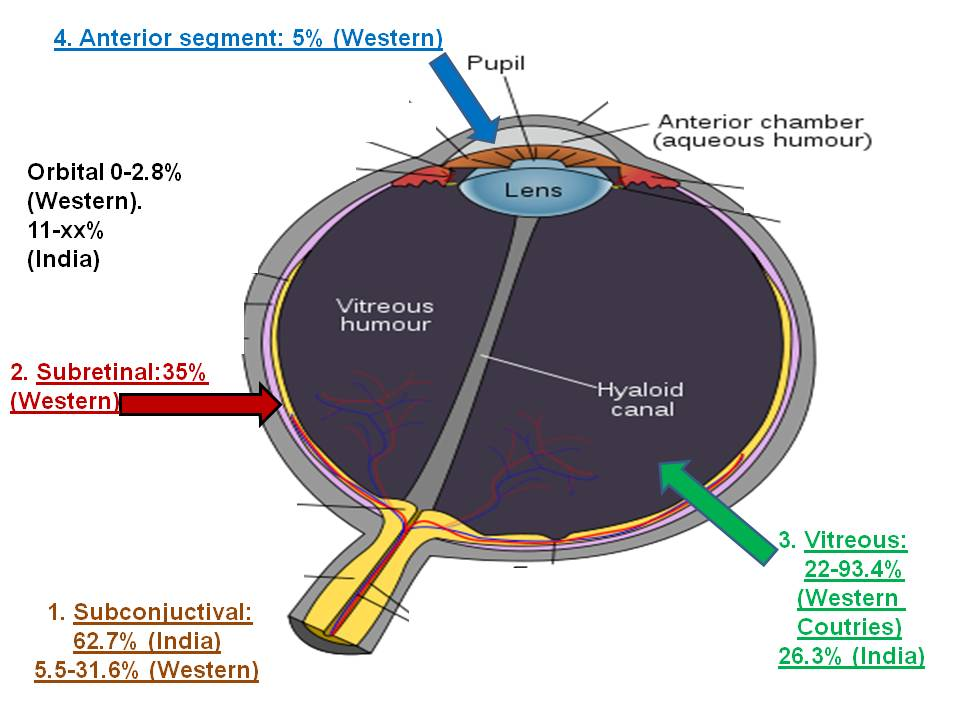
- The ocular involvement occurs in two forms: intraocular and orbital adnexal .
- The intraocular form involves anterior or posterior segments of the eye while extra-ocular muscles, subconjunctival space, eyelid, optic nerve, and retro-orbital space are involved in the orbital adnexal form.
- In the orbital adnexal form, the extra-ocular muscles are most readily involved, followed by the subconjunctival space . Among the extra-ocular muscles, the most common reported site is superior rectus.
- Orbital and adnexal cysticercosis shows predilection for children and young adults with no sex predilection
- Moreover, solitary involvement of one of the extraocular muscles is rare.
- Patients with involvement of extra-ocular muscles present with non-specific symptoms like recurrent swelling, lid edema, disturbed ocular motility, and proptosis.
- The intra-ocular form is usually readily diagnosed owing to its obvious visibility on a basic slit-lamp examination and the commonest symptom being vision loss, the diagnosis of extra-ocular muscle cysticercosis remains tricky and requires a high clinical index of suspicion
IMAGING FINDINGS
- USG
Initial modality of evaluation as it is cheap, readily available, and possesses no risk of radiation to the patient. In cases of extraocular muscle involvement ultrasound usually reveals an enlarged muscle with a cyst and scolex within. - CT
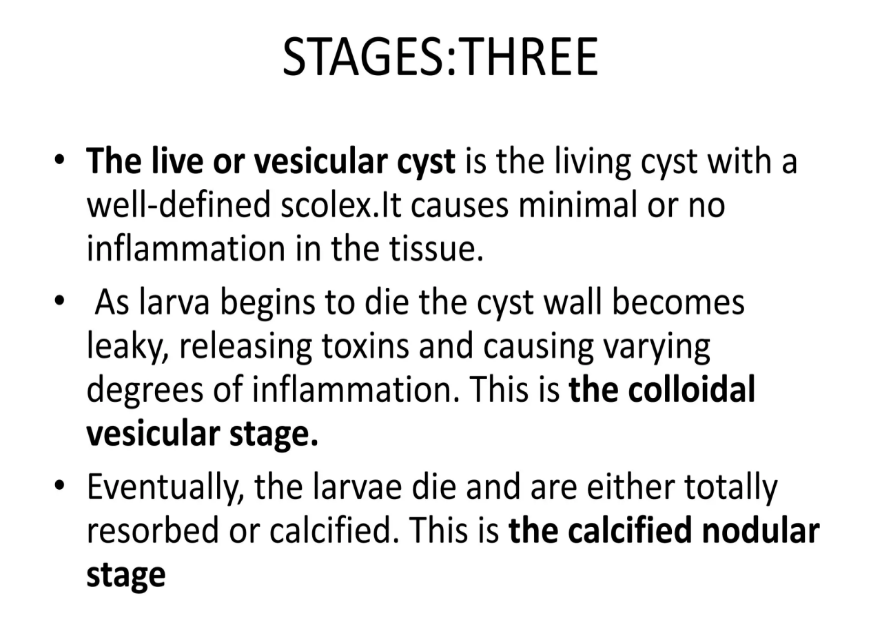
The lesion is usually seen as a hypodense mass with focal hyperdensity representing the scolex. The involved muscle appears bulky and surrounding inflammatory stranding may be present. In the calcified nodular stage, an isolated calcified granuloma-like lesion may be seen with or without any inflammatory changes - MR
A well-defined round to oval cystic lesion within the involved extra-ocular muscle, with a tiny enhancing mural nodule within the cyst
MANAGEMENT
- Conservative management in the form of an antihelminthic agent under cover of a steroid drug is initially tried before resorting to surgical management.
- Oral albendazole to be prescribed at a rate of 15 mg/kg body weight which has shown significant improvement in patient condition especially in cases of extraocular cysticercosis
- However, a close follow-up is recommended during the course of the treatment for the possibility of any adverse events .
- Surgical excision of the cyst has also been described, though the method itself is challenging and also poses a risk of increased fibrotic response and consequent restricted ocular motility
REFERENCES
- Ocular cysticercosis. Malik SRK, Gupta AK, Choudhry S. Am J Ophthalmol. 1968;66:1168–1171.
- Cystic lesions of the extraocular muscles. Sekhar GC, Lemke BN, Singh SK. Ophthalmic Plast Reconstr Surg. 1996;12:199–205.
- Extraocular muscle cysticercosis - a clinical challenge to the ophthalmologists. Sundaram PM, Jayakumar N, Noronha V. Orbit. 2004;23:255–262.
- Infestation of extraocular muscle by cysticercus cellulosae. DiLoreto DA, Kennedy RA, Neigel JM, Rootman J. Br J Ophthalmol. 1990;74:751–752.
- Orbital and adnexal cysticercosis. Pushker N, Bajaj MS, Betharia SM. Clin Exp Ophthalmol. 2002;30:322–333.
Dr. HARSHA CHADAGA
SENIOR CONSULTANT & HEAD OF RADIOLOGY
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU
Dr. MAYANK RANGARI
FELLOW IN CROSS SECTIONAL IMAGING
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU