
A 38-year-old with the history of epigastric pain with vomiting.
A 38-year-old with a history of epigastric pain with vomiting.
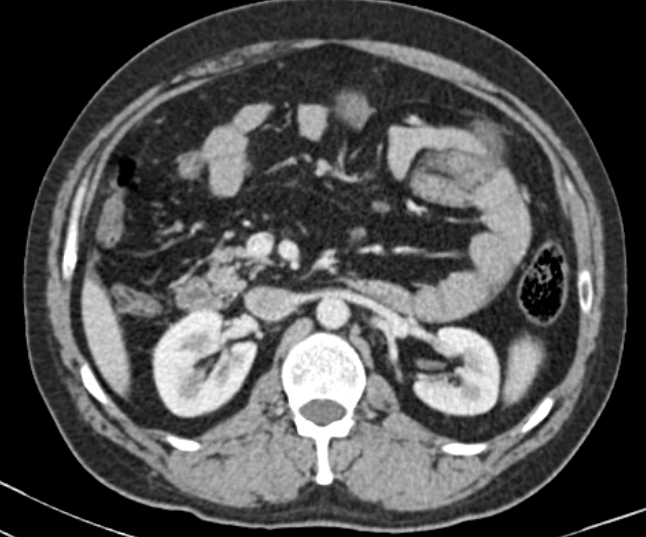
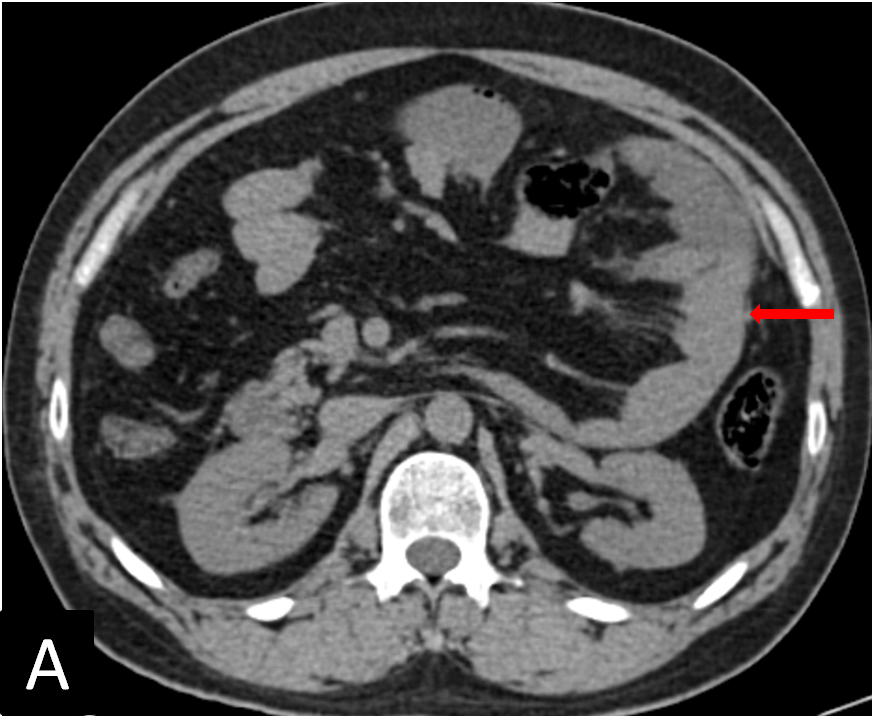
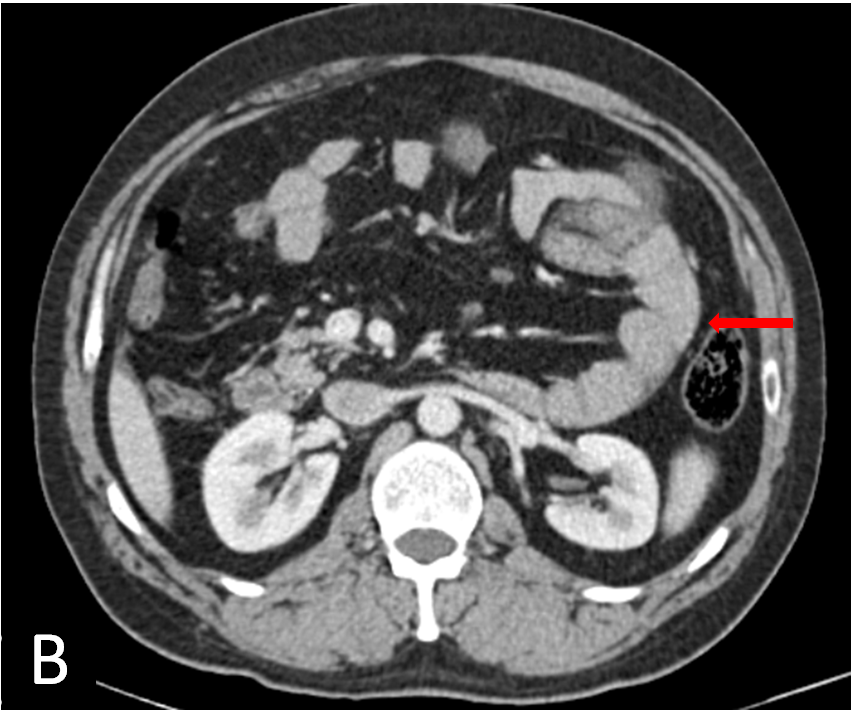
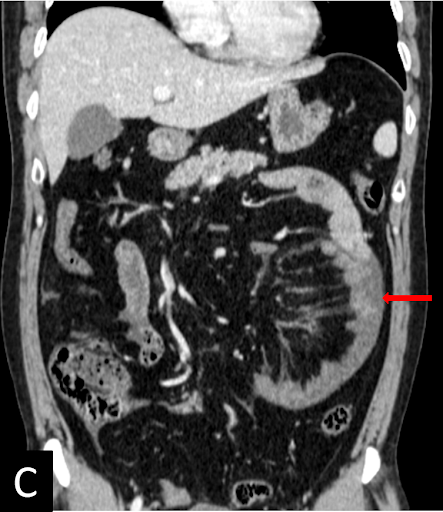
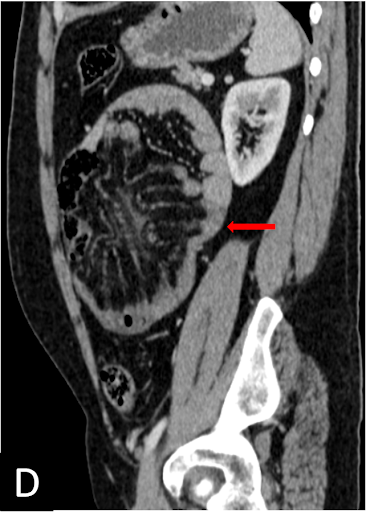
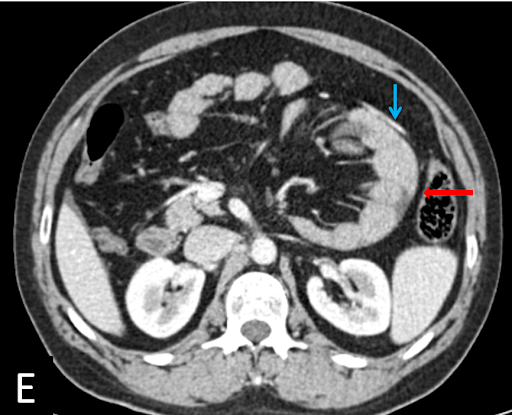
FINDINGS




DIAGNOSIS:
Left paraduodenal internal hernia.
DISCUSSION:
Internal hernias:
- Internal hernias involve protrusion of the viscera through the peritoneum or mesentery and into a compartment in the abdominal cavity.
- The most common presentation is an acute intestinal obstruction of small bowel loops that develops through normal or abnormal apertures.
- The responsible hernial orifices are usually pre-existing anatomic structures, such as foramina, recesses, and fossae. Pathologic defects of the mesentery and visceral peritoneum, which are caused by congenital mechanisms, surgery, trauma, inflammation, and circulation, are also potential herniation orifices.
- Internal hernias are silent if they are easily reducible, but the majority often cause epigastric discomfort, periumbilical pain, and recurrent episodes of intestinal obstruction.
- Internal hernias are clinically apparent only when incarcerated internal hernias result from small bowel obstruction (SBO); therefore, a delay in diagnosis may lead to strangulation and an increased risk of serious complications.
- Internal hernias are divided into three categories on the basis of the type of hernia orifice: (a) normal foramen, (b) unusual peritoneal fossa or recess into the retro peritoneum, and (c) abnormal opening in a mesentery or peritoneal ligament.
- A saclike appearance strongly supports a diagnosis of internal hernia. Unfortunately, this sign is not observed in all types of internal hernias. A saclike appearance can be observed with internal hernias into an unusual fossa in the retro peritoneum or with intramesenteric-type internal hernias.
- Definitive diagnosis of internal hernias requires identification of abnormal displacement of surrounding structures and key vessels around the hernia orifice and hernia sac.

Diagnostic approach of internal hernias with multidetector CT:
Step-A: Detect an Intestinal closed loop.
Step-B: Identify the hernia orifice.
Step-C: Analyse displacement of surrounding structures and key vessels.
Left para duodenal hernia:
- Left paraduodenal hernias are entrapments of the small bowel loops into the fossa of Landzert, an unusual congenital peritoneal fossa behind the descending mesocolon.
- This fossa results from failure of part of the descending mesocolon to fuse with the posterior parietal peritoneum.
- A cluster of intestinal loops with a saclike appearance is observed in the left anterior pararenal space.
- The inferior mesenteric vein and ascending left colic artery are landmarks situated at the anteromedial edge of the fossa of Landzert.

REFERENCES:
- Takeyama N, Gokan T, Ohgiya Y, Satoh S, Hashizume T, Hataya K, Kushiro H, Nakanishi M, Kusano M, Munechika H. CT of internal hernias. Radiographics. 2005 Jul;25(4):997-1015.
- Doishita S, Takeshita T, Uchima Y, Kawasaki M, Shimono T, Yamashita A, Sugimoto M, Ninoi T, Shima H, Miki Y. Internal hernias in the era of multidetector CT: correlation of imaging and surgical findings. Radiographics. 2016 Jan;36(1):88-106.
- Reddy UD, Dev B, Santosham R. Internal hernias: surgeons dilemma-unraveled by imaging. Indian Journal of Surgery. 2014 Aug;76(4):323-8.
Dr. Surendra K L
DMRD, DNB, FRCR, EDIR
Junior Consultant- Radiology
Manipal Hospitals Radiology Group
Dr. Bhupendar Singh
Radiology Resident,
Manipal Hospitals Radiology Group.
