
A 37 years old gentleman came with complaints of pain in left groin radiating to thigh for the past 4 months
- Patient complains of absence of left leg sensation for few minutes, after getting up from a prolonged rest. Later he is able to walk normally.
- No back pain, no difficulty in walking, no bowel or bladder symptoms, no incontinence, no upper limb symptoms.
FINDINGS:
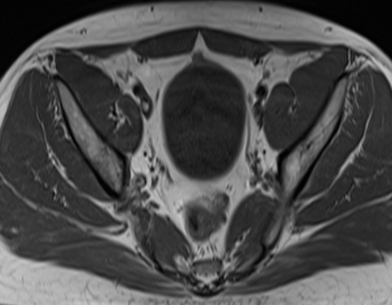
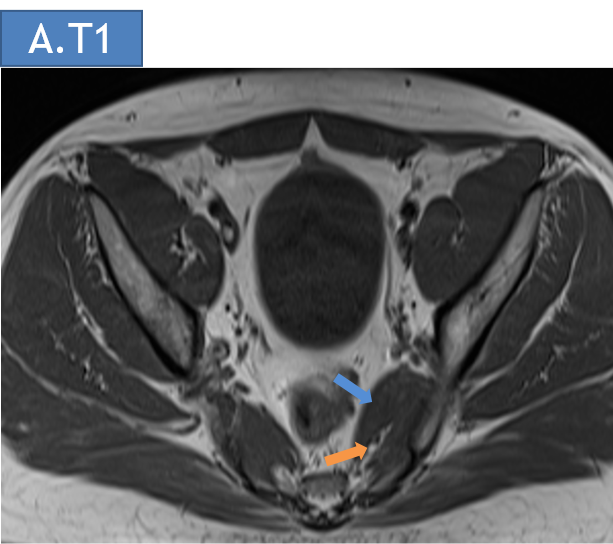
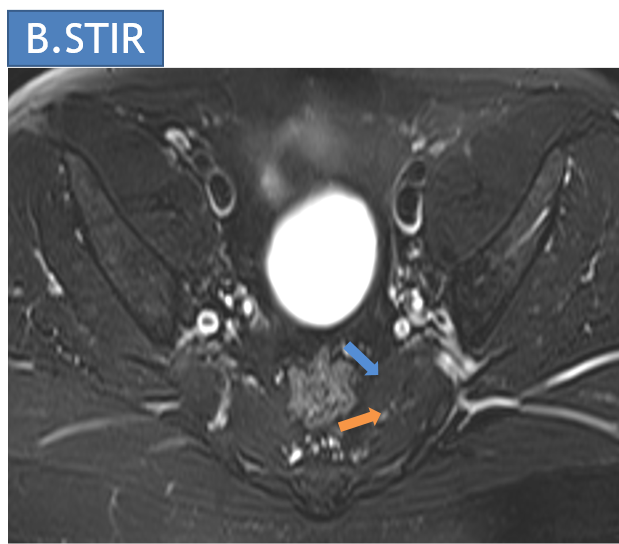
- Axial T1 and STIR images of pelvis at the level of sciatic notch
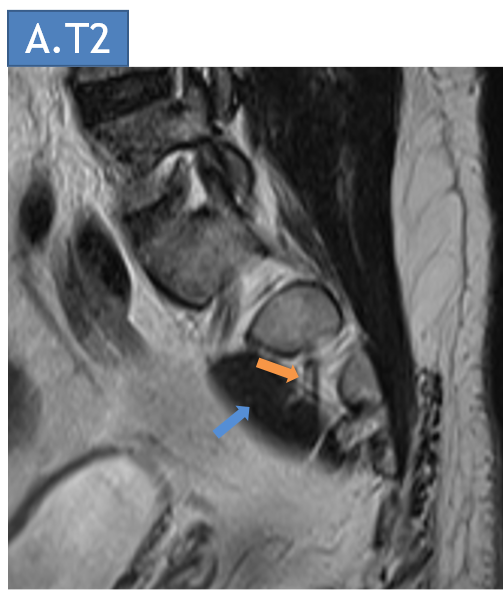
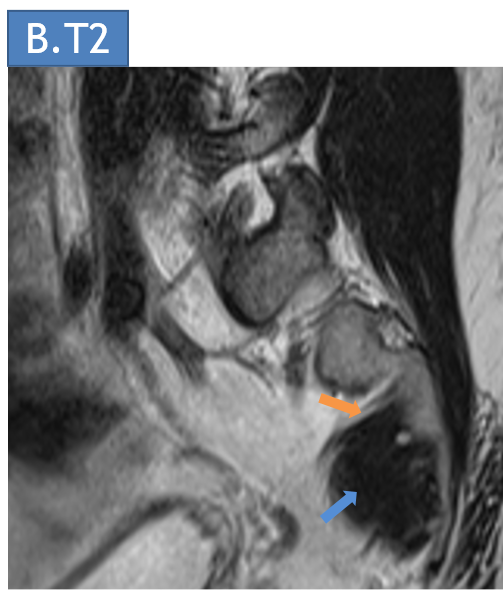
- T2.1 & T2.2: Sagittal T2 weighted images of the pelvis in the right and left paramedian aspect
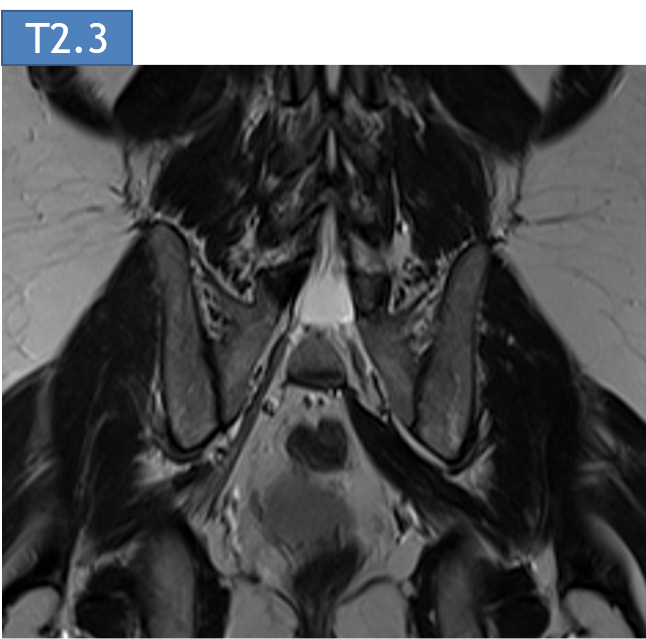
- T2.3: Coronal T2 weighted image of the pelvis
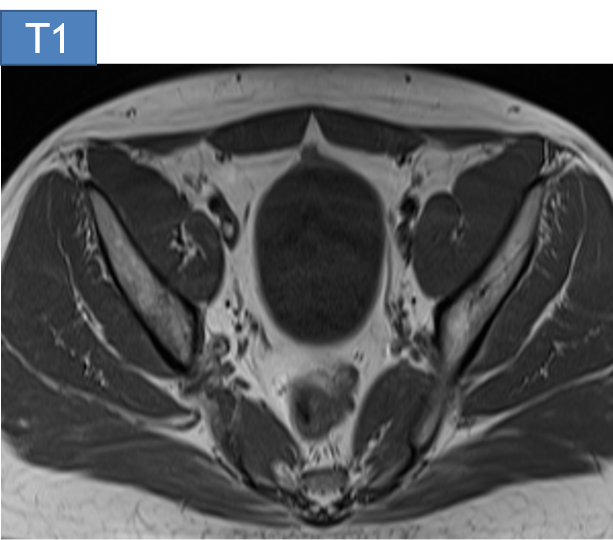


Axial T1 and STIR images of pelvis at the level of sciatic notch
- (a) Axial T1-weighted MRI of the pelvis at the level of the sciatic notch demonstrates the left S1/2 exiting nerve root(orange arrow) being compressed by the accessory slip of the left piriformis muscle(blue arrow)
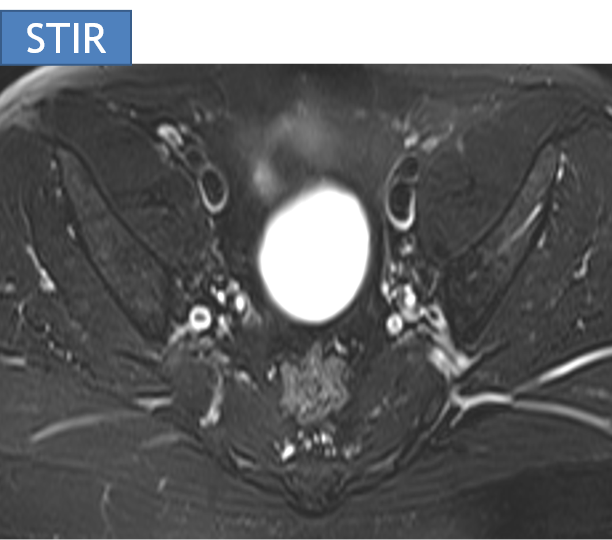
- (b) Axial STIR images of the pelvis at the level of the sciatic notch demonstrates the left S1/2 exiting nerve root (orange arrow) being compressed by the accessory slip of the left piriformis muscle(blue arrow).
Sagittal T2 weighted images of the right and left paramedian aspect of the sacrum
- (a) Sagittal T2 MRI of the left paramedian aspect of the pelvis demonstrating the S1/2 exiting nerve root (orange arrow) being compressed by the accessory slip of the left piriformis muscle (blue arrow)
- (b) Sagittal T2 MRI of the right paramedian aspect of the pelvis demonstrating the normal anatomical relationship between the S1/2 exiting nerve root(orange arrow) and the piriformis muscle (blue arrow). The S1/2 exiting nerve root is superior and anterior to the piriformis.
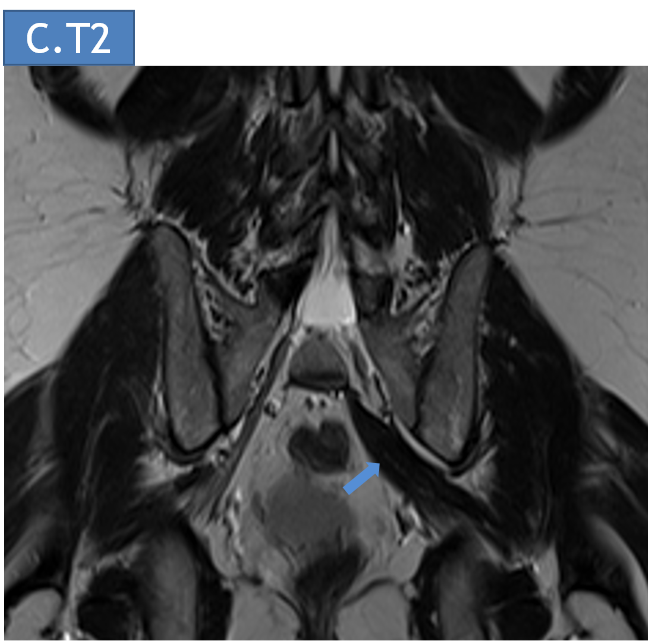
Coronal T2 weighted image of the pelvis
- (c) Coronal T2 MRI of the pelvis demonstrating the accessory slip of the left piriformis muscle (blue arrow)
DIAGNOSIS:
Bulky left pyriformis muscle with an accessory slip - Piriformis syndrome
DISCUSSION:
Piriformis syndrome
- Piriformis syndrome is a rare entrapment neuropathy resulting in radicular pain radiating into the buttock and hamstrings.
- It is caused when hypertrophy, inflammation, injury or anatomical variation of the piriformis muscle results in compression of the sciatic nerve as they both exit the pelvis through the greater sciatic notch.
- Normally, the sciatic nerve typically passes immediately anterior to the piriformis muscle. This relationship is variable, however, as the nerve occasionally passes through the muscle, or splits early, with part of it passing through the muscle.
- Additionally, an accessory piriformis muscle that arises from the more medial part of the sacrum can be implicated.
Beaton and Anson classification of different anatomical relationships between the sciatic nerve and piriformis muscle and their estimated prevalence.
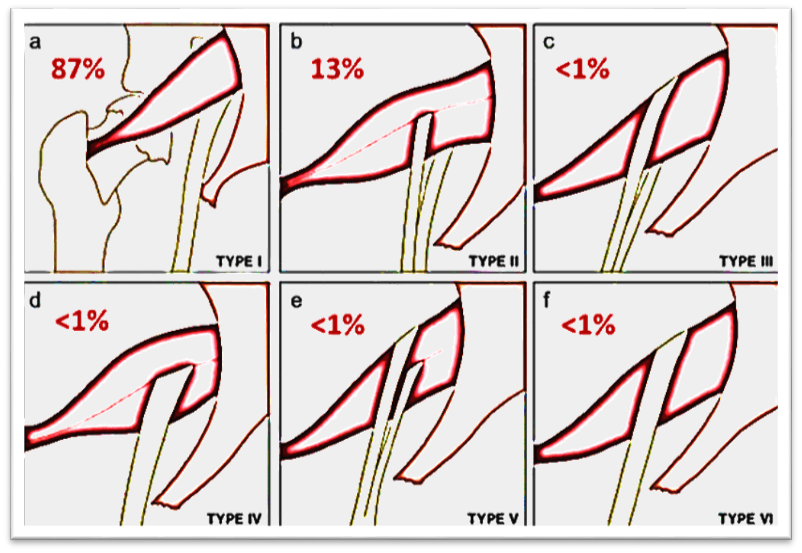
(a) Type 1: undivided sciatic nerve passing anterior and below the piriformis. (b) Type 2: common peroneal nerve component piercing a bifid piriformis, tibial component running in normal position anterior and inferior to piriformis. (c) Type 3: one division posterior to and the other anterior to the piriformis. (d) Type 4: undivided sciatic nerve piercing bifid piriformis. (e) Type 5: one division through and the other posterior to the piriformis. (f) Type 6: undivided nerve posterior to piriformis. Figure courtesy : Varenika et al.
Normal anatomical relationship between the sciatic nerve and the piriformis muscle
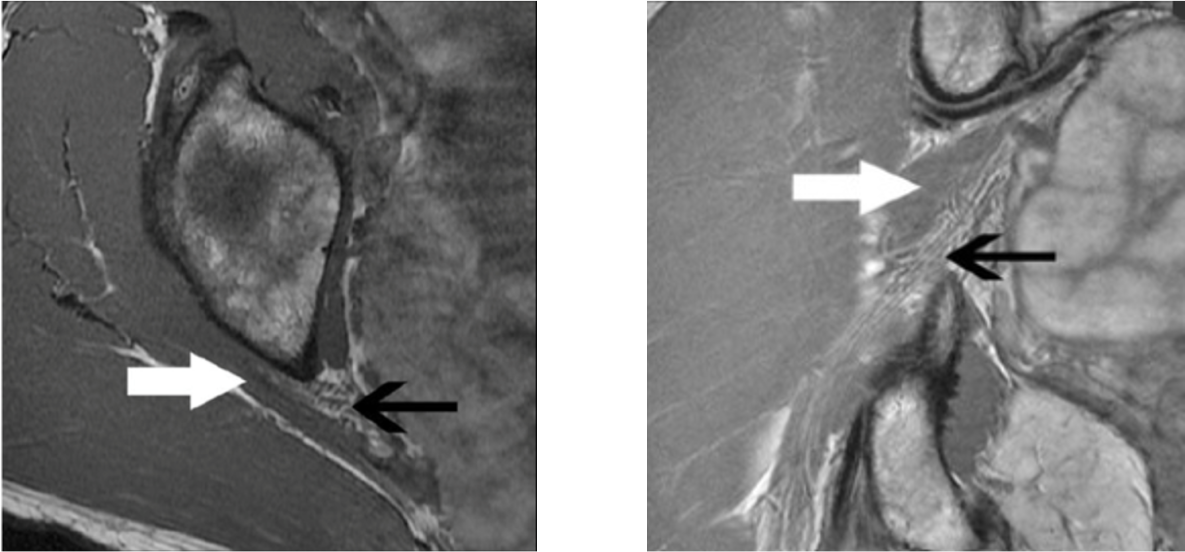
(a) Axial T1-weighted MRI of the sciatic nerve at the level of the sciatic notch demonstrates normal sciatic nerve (black arrow) anterior to the piriformis (white arrow). (b) Coronal T1-weighted sequence showing type I sciatic nerve (black arrow) inferior to the piriformis (white arrow).
Gross anatomy of the piriformis
- It is situated partly within the pelvis against its posterior wall, and partly at the back of the hip joint.
Origin
- The piriformis muscle originates from the anterior part of the sacrum by three fleshy digitations (middle three pieces of its own half and adjoining lateral mass, and also extending medially between the anterior sacral foramina) as well as from the superior margin of the greater sciatic notch, and to a lesser extent the sacroiliac joint capsule and the sacrotuberous ligament.
Course
- The muscle passes out of the pelvis through and fills the upper part of, the greater sciatic foramen into the gluteal region.
Insertion
- The piriformis exits the pelvis through the greater sciatic foramen to insert on the apex of the greater trochanter of the femur.
Its tendon often joins with the tendons of the superior gemellus, inferior gemellus, and obturator internus muscles prior to insertion.
Accessory piriformis muscle:
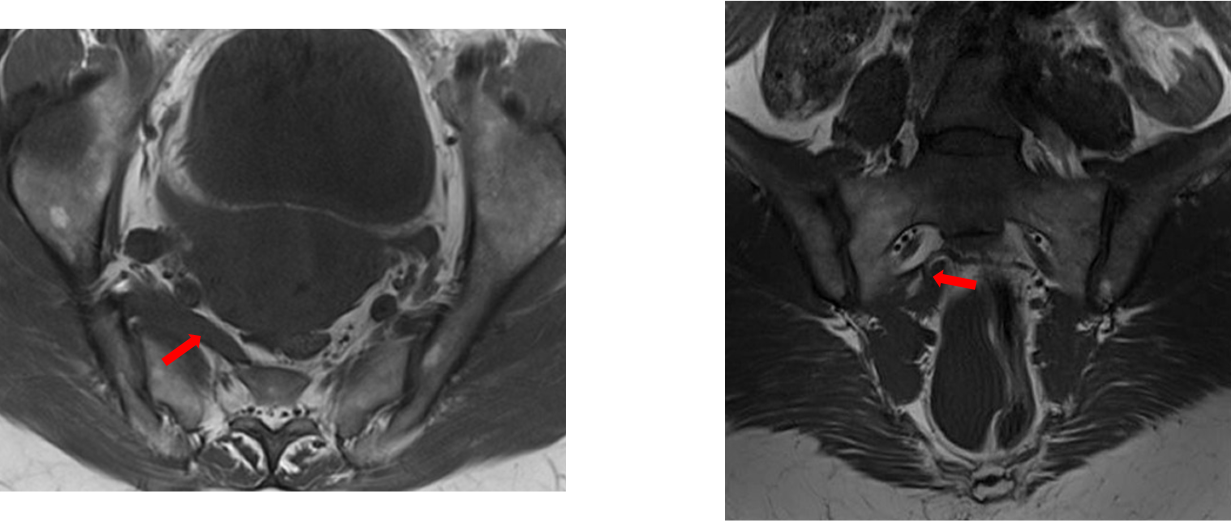
Right accessory piriformis muscle(red arrow) which crosses over the right sacral foramen.The right S2 nerve passes between this accessory muscle and the proper right piriformis muscle, without significant compression or nerve or muscle oedematous changes.
Accessory piriformis muscle variations
An accessory piriformis muscle, which is really accessory muscle slip(s), has considerable variability:
- Accessory muscle slips covering sacral foramina / sacral nerves.
- Two distinct muscle bellies fusing to form a common tendon.
- Accessory slips arising from the sacrotuberous ligament or gluteus medius fascia
- Three muscle bellies.
- Accessory slip arising from the main muscle belly with a separate tendinous insertion into the greater trochanter.
Clinical Diagnosis:
- Freiberg described tests that recreate the patients pain referable to the piriformis muscle, felt to be diagnostic of entrapment:
- Lasegue’s sign - Pain at sciatic notch with extension of the knee while the hip is flexed to 90 degrees, and tenderness to palpation at the sciatic notch
- Freiberg’s sign - Pain with passive internal rotation of the hip.
- Pace’s sign has also been described - pain and weakness in association with resisted abduction and external rotation of the affected thigh.
- These signs were helps to differentiate piriformis syndrome from other cause of radicular pain such as disc herniation, extrinsic pressure by tumor or other mass, or intrinsic nerve abnormality.
Etiology of piriformis syndrome
Early sciatic nerve division and passage through the muscle belly or above it
Narrowed sciatic foramen
- Accessory piriformis muscle
- Muscle hypertrophy
- Lumbar lordosis
- Ganglion or cyst
- Any mass lesion
Spasm
- Athletes
- Cerebral palsy
Bursitis and inflammation
Role of imaging in piriformis syndrome
- The findings on imaging studies are variable and depends on the cause, and often no abnormality is noted.
- The most common finding on MRI or CT is asymmetry of the piriformis muscle, most often hypertrophy, but sometimes atrophy of the muscle on the affected side.
- Abnormal increased radiotracer uptake by the piriformis muscle on the affected side has been reported on bone scan.
- In the case of myositis ossificans, x-ray, bone scan and MRI will all have diagnostic value.
- In the case of anatomic variation such as an accessory head of the piriformis muscle, the superior soft tissue detail of MRI will be most useful for diagnosis.
- Since the symptoms of piriformis syndrome and lumbosacral disc herniation are often difficult to distinguish, and intraspinal etiologies are, after all, far more common, many patients undergo lumbar spine MRI first.
- Once causes of radicular symptoms have been excluded by MRI or CT myelogram, an MRI of the pelvis is useful in cases where physical exam is suggestive of piriformis syndrome, since asymmetry of the muscles, if found, is highly suggestive of the diagnosis.
Treatment:
- Physiotherapy with stretching (especially if a spasm is thought to be the cause)
- Administration of non-steroidal anti-inflammatory agents
- Injection of local anaesthetic and steroid
- Injection of botulinum toxin to atrophy the piriformis muscle
- Surgical release of the piriformis muscle.
- Neurolysis
Dr. Deepti H V
Senior Consultant
Department of Radiology
Manipal hospital, Yeshwanthpur, Bengaluru.
Dr. Ram Sanjith V
Cross Section Fellow
Department of Radiology
Manipal hospital, Yeshwanthpur, Bengaluru.
