

A 36 year old gentleman with history of left chest pain
A 36-year-old gentleman with a history of left chest pain.


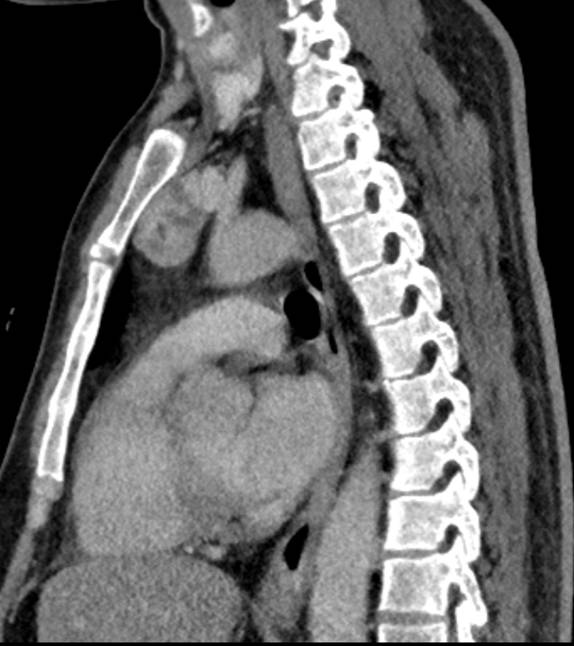

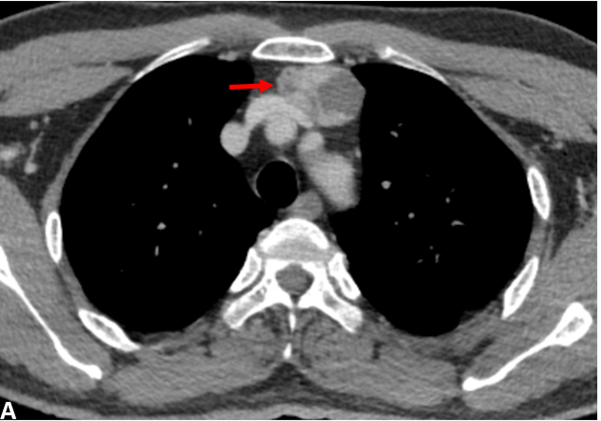
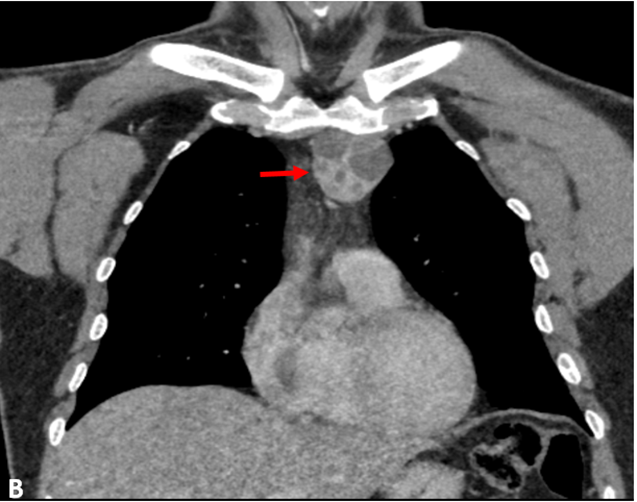
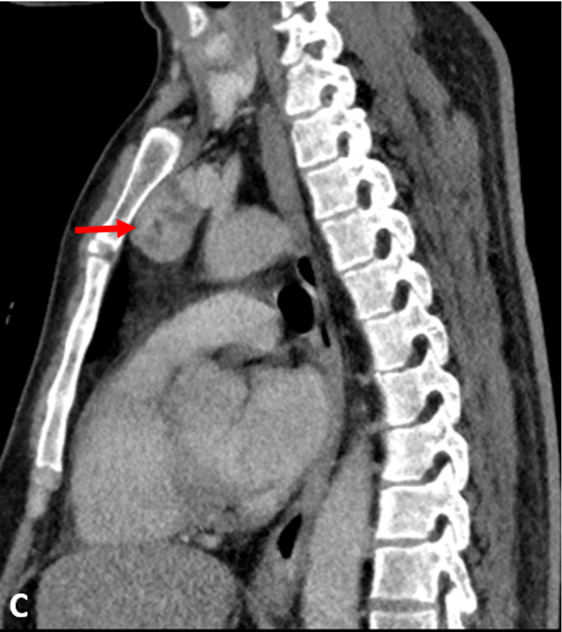
- Axial (A), Coronal (B) and Sagittal (C) CECT Chest demonstrates a well-circumscribed solid-cystic, retrosternal mass lesion in superior mediastinum, immediately posterior to manubrium sternum. No fatty elements. Superiorly thyroid gland separately visualized from the lesion (C).
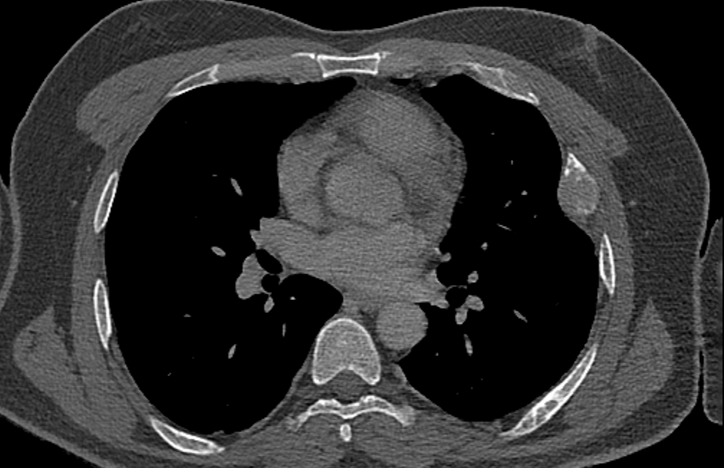
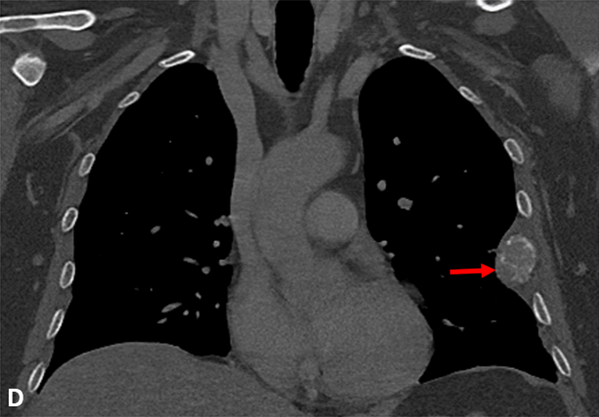
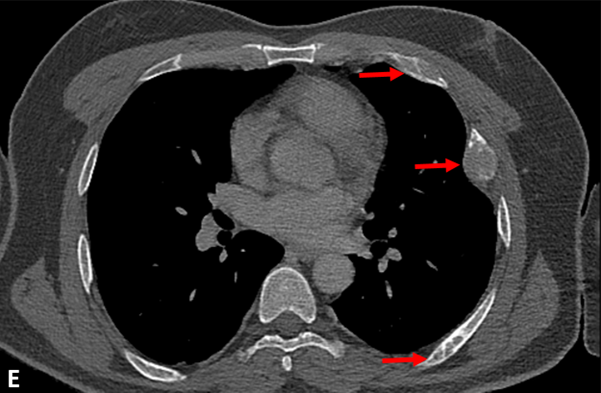
- Coronal (D) and Axial (E) CT-Chest bone window demonstrates multiple expansile lytic lesions in left side ribs.
Diagnosis:
Ectopic parathyroid adenoma with brown tumors of ribs.
Discussion:
- Hyperparathyroidism can be due to primary, secondary and tertiary causes.
- Primary hyperparathyroidism is characterized by high parathyroid and calcium levels which is most commonly due to a parathyroid adenoma.
- Symptoms of hypercalcemia range from osteoporosis, vomiting, constipation, calculus, polyuria and polydipsia.
- Acute pancreatitis, kidney damage and involvement of the bone are major long-term complications of primary hyperparathyroidism.
- Involvement of bone can be in the form of generalized demineralization, focal lytic lesion or sub periosteal resorption. Ectopic parathyroid adenomas have increased risk of bone involvement compared to others.
Ectopic Parathyroid Adenoma:
- Ectopic parathyroid glands are most often derived from inferior glands. They may be located in the mediastinum either anterior or posterior, in the thymus (intrathymic), in the tracheoesophageal groove and very rarely in the thyroid parenchyma.
- Pre-operative localisation of the hyper functional parathyroid adenoma is crucial for successful and minimally invasive parathyroidectomy.
- Pre-operative anatomical localisation of the parathyroid glands may be achieved by USG, CT and MRI.
- Functional localisation modalities include dual-isotope imaging with or without Single-photon emission CT (SPECT)-CT using 99mTc-sestamibi (MIBI)/99mTc-pertechnate.
- Newer techniques such as hybrid localisation with newer tracer agents such as 11C-choline or 18F-fluorocholine or 14C methionine PET-CT and 4D CT.
Imaging differentials:
- Thymoma
- Teratoma (germ cell).
- Thyroid neoplasm / thyroid goiter.
- Terrible Lymphoma.
References:
- Panchani R, Varma T, Goyal A, Gupta N, Saini A, Tripathi S. A challenging case of an ectopic parathyroid adenoma. Indian J Endocrinol Metab. 2012 Dec; 16(Suppl 2):S408-10.
- Harinarayan, C. V., et al. “Ectopic parathyroid adenoma: single-centre experience from India.” Journal of Clinical and Scientific Research 7.2 (2018): 69.
- Elhelf, Islam A Shehata et al. “Ectopic mediastinal parathyroid adenoma localized with four-dimensional CT: a case report.” Radiology case reports vol. 12,2 247-250. 20 Feb. 2017, doi:10.1016/j.radcr.2017.01.011.
Dr. Pravin Kumar M,
Consultant Radiologist,
Manipal Hospitals Radiology Group.
Dr. Bhupender Singh,
DNB Resident,
Manipal Hospitals Radiology Group.

