
A 26-year-old with complaints of increased menstrual bleed associated with increased abdominal pain
A 26-year-old with complaints of increased menstrual bleeding associated with increased abdominal pain
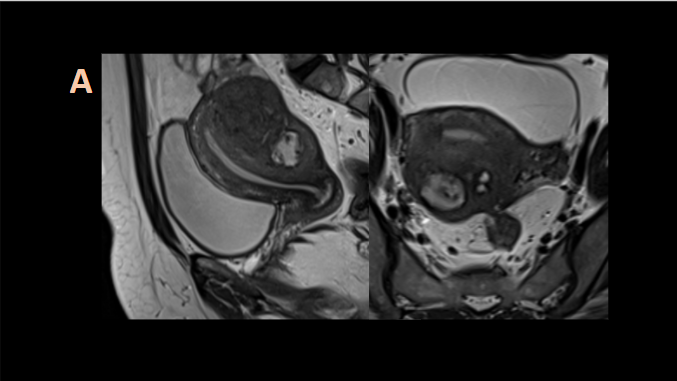
A .Sagittal and axial T2W images show thickened posterior myometrium with heterogenous T2 hypointensity with scattered and confluent areas of T2 hyperintensity. Endometrium is normal.
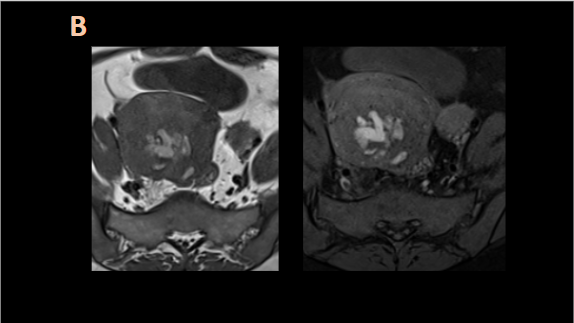
B. Axial T1 and fat suppressed T1W images confirm areas of haemorrhage in the thickened posterior myometrium.
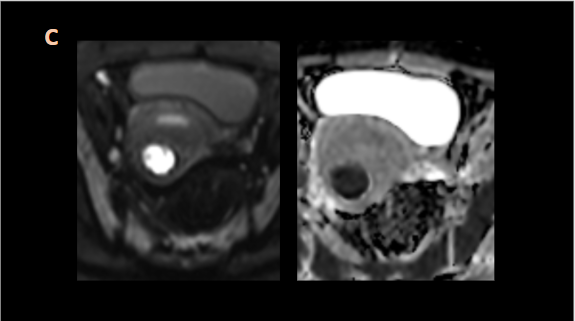
C. The larger foci show diffusion restriction with low ADC values.
DIAGNOSIS:
Adenomyosis with haemorrhage
DISCUSSION:
ADENOMYOSIS
- Adenomyosis occurs mainly in premenopausal women, particularly those who are multiparous. In postmenopausal women, tamoxifen is known to increase the incidence of adenomyosis.
- It is non neoplastic condition, pathologically characterized by benign invasion of ectopic endometrium into the myometrium with adjacent smooth muscle hyperplasia. Endometrial glands lying deeper than one-fourth of the thickness of the myometrium or deeper than one-half of a low-power field (about 2.5 mm) are defined as adenomyosis on histopathology.
- Common symptoms include dysmenorrhea, menorrhagia, and abnormal uterine bleeding.
- Associations include co-existent endometriosis, leiomyomas(~50%) involving adenomyosis of the uterus, endometrial hyperplasia and endometrial polyps.
- Treatment for adenomyosis depends on the patient’s symptoms, age, and desire for future fertility. The definitive treatment is hysterectomy, but initially less invasive approaches like NSAIDs, GnRH analogues, drug eluting IUDs are tried in young.
IMAGING
- TAS or TVS is commonly used as the initial imaging modality. Typical appearances of adenomyosis at TVS include poorly marginated hypoechoic and heterogeneous areas within the myometrium, myometrial cysts, and a globular or enlarged uterus with asymmetry.
- MR imaging is an accurate, noninvasive modality with a high sensitivity (78%–88%) and specificity (67%–93%) . It is more helpful than TVS in delineating the location & extent of the lesion;in monitoring the evolution of disease in patients receiving hormonal therapy and also in distinguishing adenomyosis from a leiomyoma.
- Adenomyosis appears as either diffuse or focal thickening of the junctional zone forming an ill-defined area of low signal intensity, occasionally with embedded bright foci on T2-weighted images. Histologically, areas of low signal intensity correspond to smooth muscle hyperplasia, and bright foci on T2-weighted images correspond to islands of ectopic endometrial tissue and cystic dilatation of glands. When menstrual hemorrhage occurs within these ectopic endometrial tissues, T1W hyperintensities can be seen.
- In general, a maximal junctional zone thickness of more than 12 mm is highly predictive of the presence of adenomyosis.
Pseudolesions Masquerading as Adenomyosis:
- Junctional zone thickening during menstruation (especially cycle days 1 and 2)
- Sustained myometrial contraction: focal and sporadic bulging of the myometrium into the uterine cavity.
Unusual Appearances
- Adenomyoma: localized, circumscribed form, polypoid mass protruding into the cavity.
- Adenomyotic Cyst: caused by extensive menstrual bleeding into the ectopic endometrium
Differential Diagnosis of Adenomyosis
- Solid invasive endometriosis of posterior myometrium: Solid implants in endometriosis may invade the posterior myometrium and mimic adenomyosis. Review in all planes can be useful. Also, the junctional zone here is often spared.
- Leiomyoma: In contrast to leiomyoma, adenomyosis manifests with a poorly defined border, minimal mass effect, an elliptical rather than round configuration, and absence of dilated vessels at the margin of the lesion
- Adenomatoid Tumor of the Uterus: ill-defined or well-circumscribed mass of low signal intensity on T2-weighted images, an appearance that can be indistinguishable from that of leiomyoma or adenomyoma.
- Metastasis to the Uterine Corpus: most common are from breast cancer (especially invasive lobular carcinoma) and gastrointestinal cancer.
- Endometrial Stromal Sarcoma: typically appears as a polypoid endometrial mass with extensive myometrial involvement, may occasionally appear as an infiltrative myometrial lesion with only minimal involvement of the endometrium in very young women
References:
1. Tamai, K., Togashi, K., Ito, T., Morisawa, N., Fujiwara, T., & Koyama, T. (2005). MR imaging findings of adenomyosis: Correlation with histopathologic features and diagnostic pitfalls. RadioGraphics, 25(1), 21–40. https://doi.org/10.1148/rg.251045060
2. Gaillard, F., 2022. Adenomyosis | Radiology Reference Article | Radiopaedia.org. [online] Radiopaedia.org. Available at: <https://radiopaedia.org/articles/adenomyosis> [Accessed 29 January 2022].
Dr Naveen SS
DNB resident
Manipal Hospital, Yeshwanthpur
Dr Sriram Patwari, MDRD, PDCC
Senior Consultant
Manipal Hospital, Yeshwanthpur
