
A 23 year old, male presented with clear watery discharge from the left nasal cavity and history of fever, severe headache and signs of meningitis.
FINDINGS:
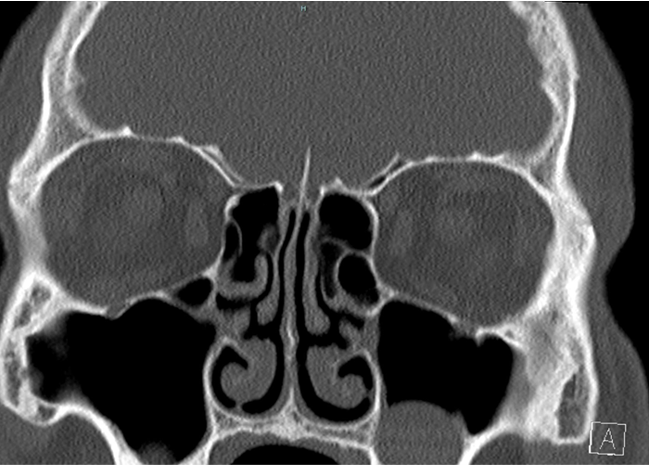
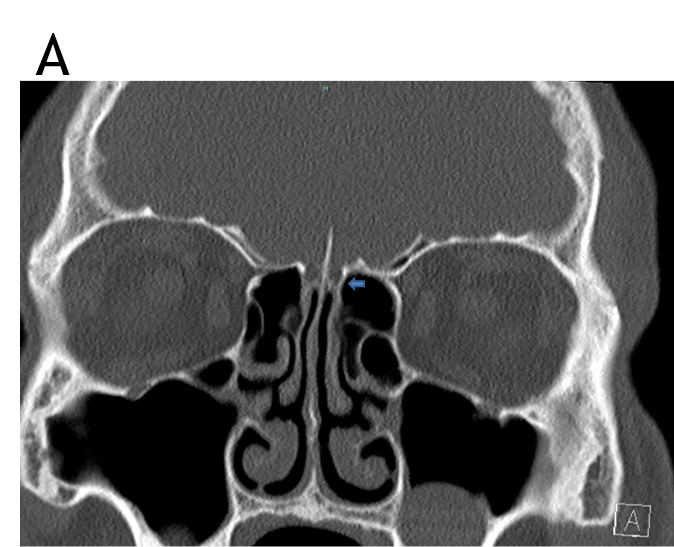
- CT-PNS coronal and sagittal views at the level of the cribriform plate and the roof of ethmoid and sphenoid sinus to evaluate the CSF leak.
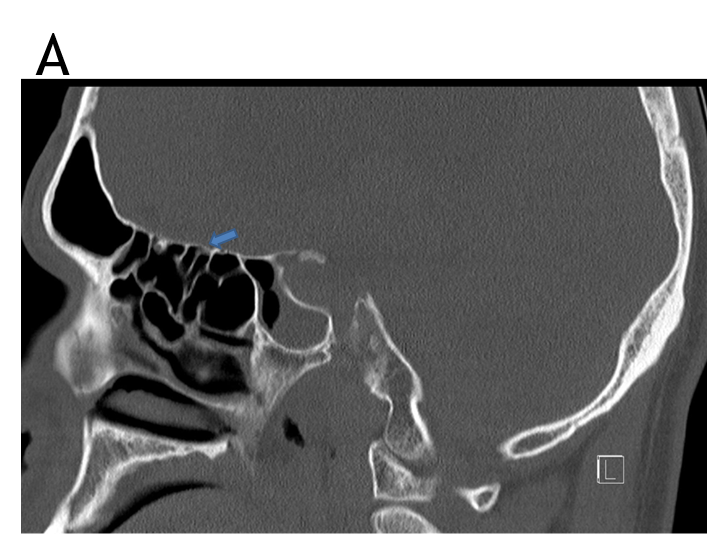
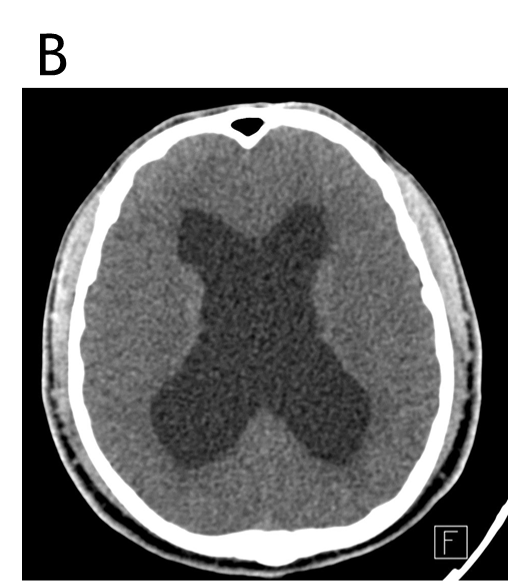
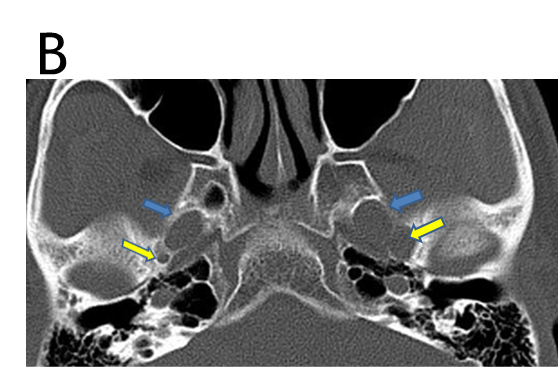
- Axial-CT brain window, axial and coronal images at the level of the neural foramina.
- CE-MRI of the brain, axial T2WI, sagittal post-contrast T1 and axial T2WI at the level of orbits.
- Coronal and axial T2W, sagittal T2W SPACE images
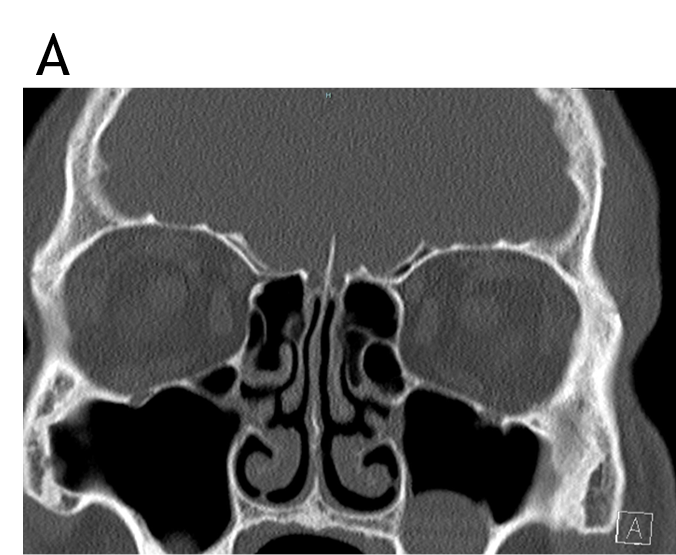
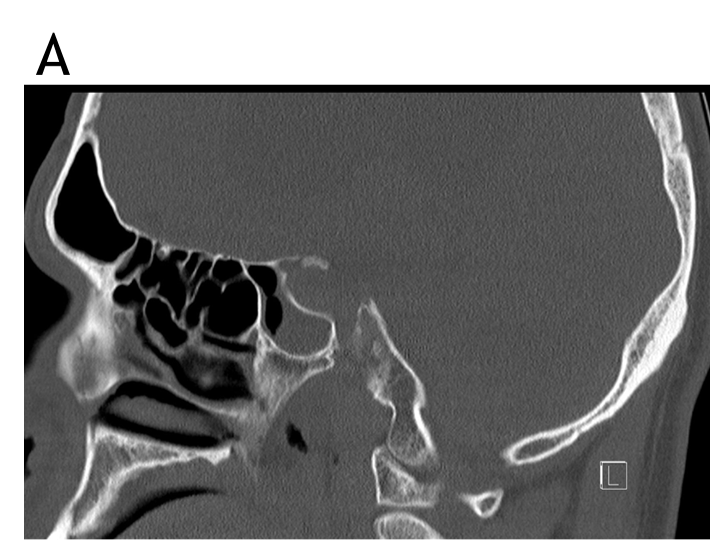




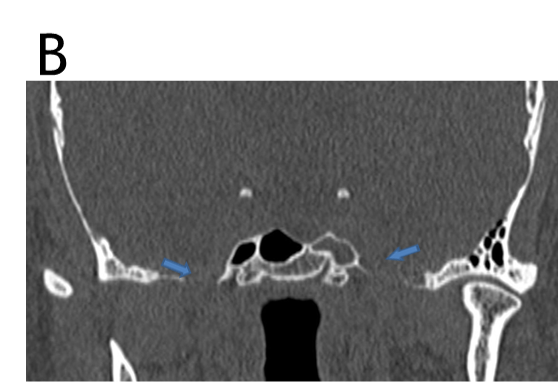
- CT-PNS coronal and sagittal views at the level of the cribriform plate and the roof of ethmoid and sphenoid sinus - No bony defect noted at the cribriform plate, roof of the ethmoid and the sphenoid sinus.
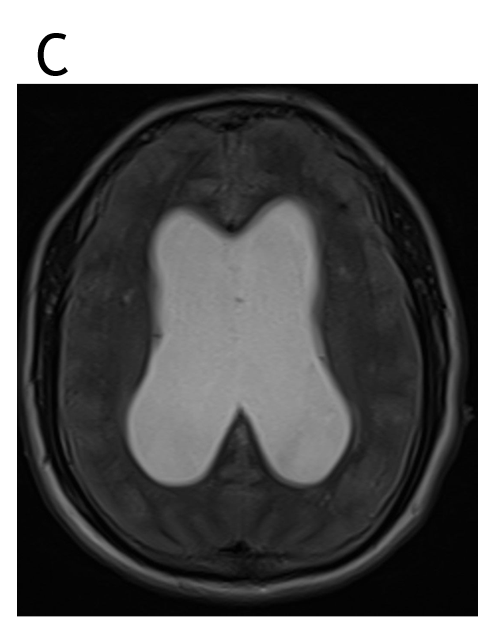
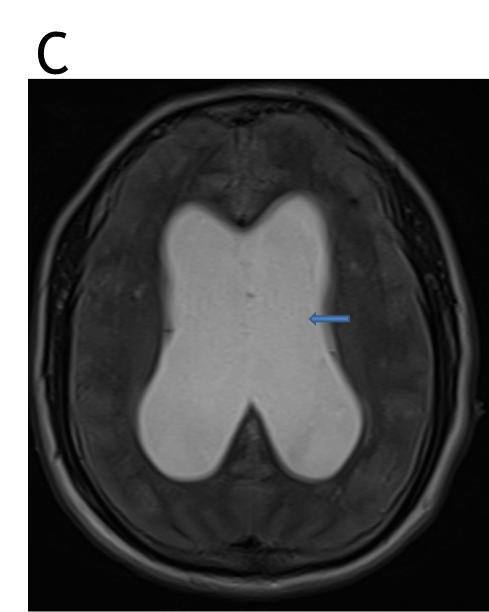
- Axial-CT brain window -Dilated bilateral lateral ventricles with mass effect in the form of effacement of sulci, Sylvian fissure.
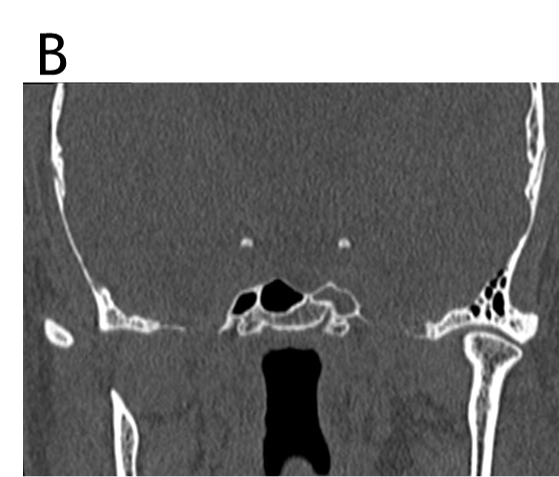
Axial and coronal images at the level of the neural foramina - Widening of neural foramina- foramen ovale (blue arrow) and foramen spinosum (yellow arrow)- left>right. - Axial T2WI - dilated bilateral lateral ventricles with mass effect in the form of effacement of sulci and fissures.
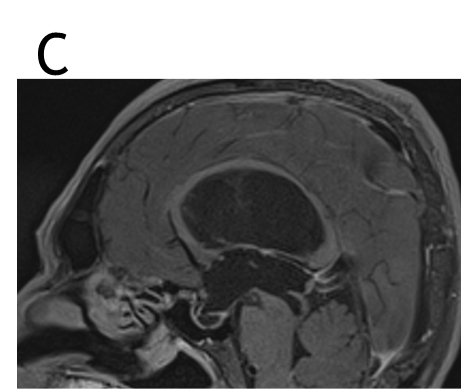
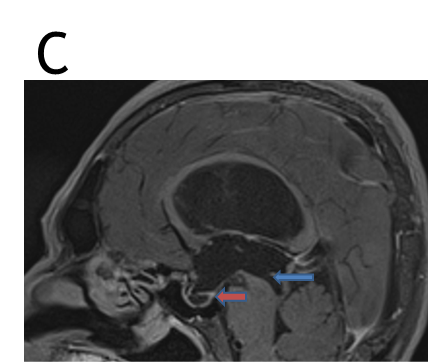
Sagittal post contrast T1 images - Dilated lateral ventricles, III ventricle (with dilated recesses of the third ventricle), partially empty sella (red arrow).
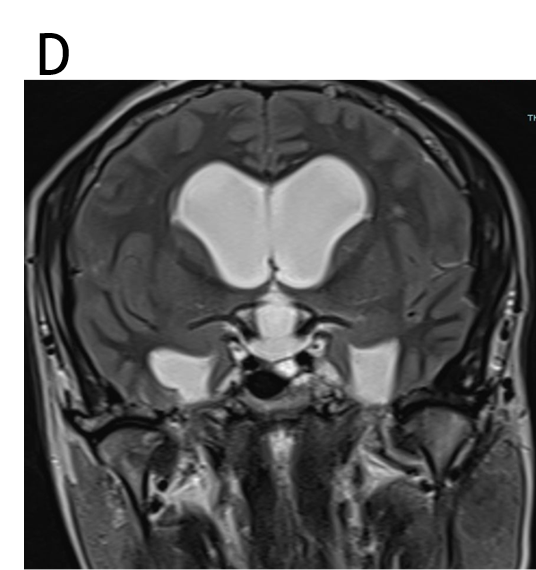
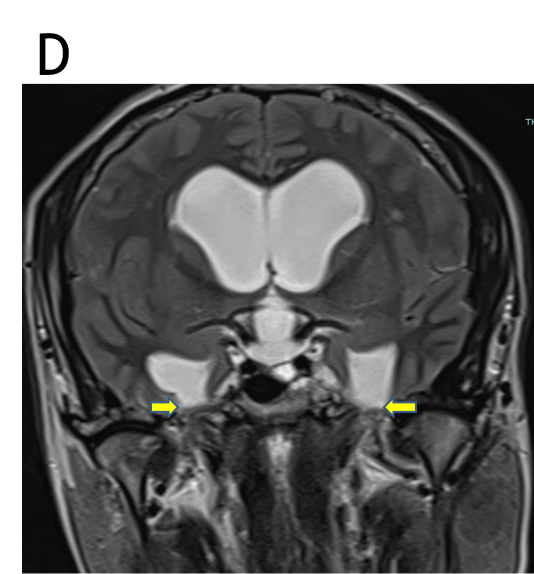
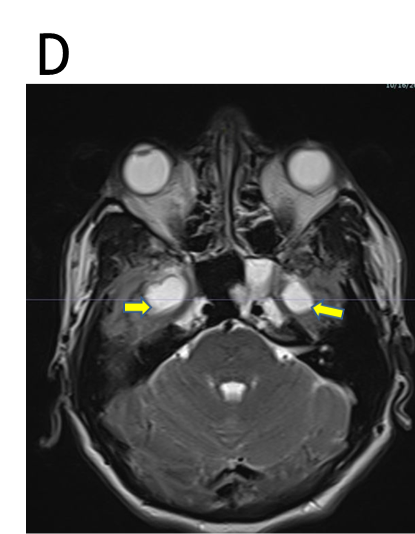
Axial T2W images at the level of orbits show tortuous course of bilateral optic nerves. - Coronal and axial T2WI show Triventriculomegaly and herniation of the temporal horns of bilateral lateral ventricles through the foramen ovale (yellow arrow). IV ventricle appears normal.
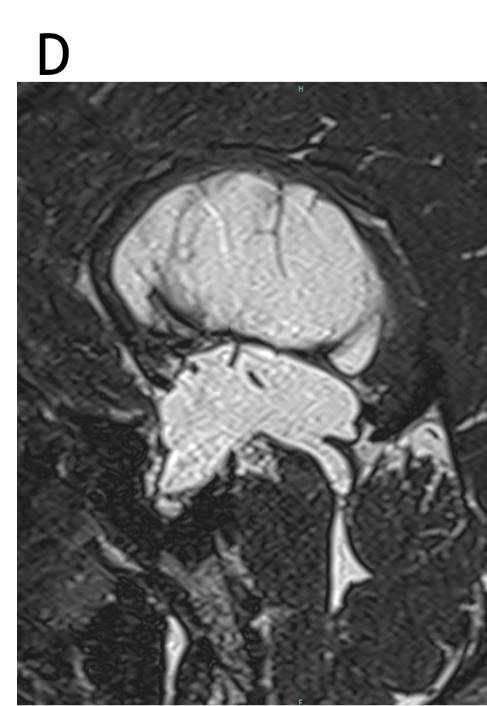
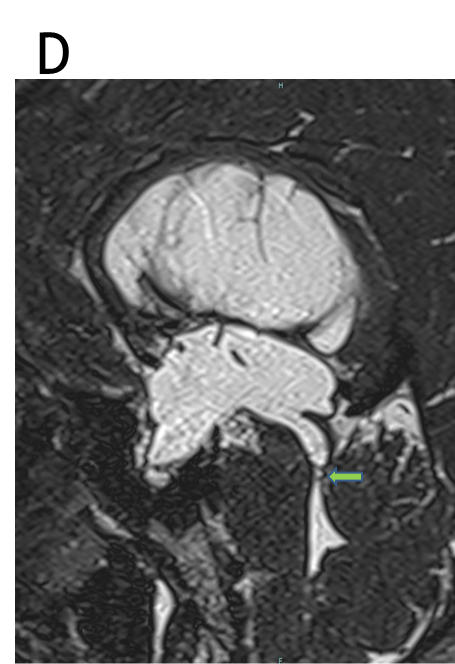
Sagittal T2W SPACE images demonstrates thin, hypointense, arachnoid webs (green arrow) at the cerebral aqueduct, with consequent aqueductal stenosis and thereby leading to hydrocephalus and features of raised intracranial pressure.

Probable etipathogenesis:
- Arachnoid webs at the cerebral aqueduct → Hydrocephalus → Increased intracranial pressure → CSF rhinorrhea → Meningitis.
DISCUSSION
- Cerebrospinal fluid (CSF) leak occurs due to a defect in the dura and skull base.
- Early diagnosis of CSF leak is important to prevent life-threatening complications such as brain abscess and meningitis.
- Trauma remains the most common cause of CSF leak, can also be iatrogenic (post-FESS).
- Non-traumatic CSF leaks include:
- Leaks secondary to tumors, infections.
- Congenital anomalies such as cephaloceles, persistent craniopharyngeal canal, or cribriform plate defect.
- Spontaneous CSF leaks / primary CSF fistulas -are commonly seen in middle-aged obese women and are associated with intracranial hypertension. - The most common site for spontaneous CSF leak is the cribriform plate followed by the ethmoid roof and can also involve the sphenoid sinus, peri-sella, or pterygoid recesses.
IMAGING:
- High resolution CT to detect the site and size of the bony defect.
- CT cisternography, though invasive, helps in accurately identifying the site of CSF leak, especially in the presence of multiple bony defects.
- MRI accurately detects CSF leaks and associated complications such as the encephaloceles and meningoceles.
Aqueductal stenosis is narrowing of the cerebral aqueduct.
It is the most common cause of congenital obstructive hydrocephalus, and can also be seen in adults as an acquired abnormality.
CLINICAL FEATURES:
- In infants - enlarged head size, bulging fontanelles and gaping cranial sutures are seen.
- Features of raised intracranial pressure and chronic hydrocephalus, including headache, vomiting, decreased conscious state may be noted.
- In adults with late-onset idiopathic aqueductal stenosis, chronic onset of neurological symptoms are noted.
- An association with Bickers Adams Edwards syndrome, a rare x-linked disorder with profound intellectual disability, adducted thumb, large head and other congenital CNS anomalies (corpus callosum agenesis, absence of the medullary pyramids, cortico-spinal tracts agenesis) is noted.
Pathology:
- Congenital
Aqueductal webs or diaphragms
Gliosis - Acquired
Infection: meningitis/ ventriculitis
Tumours: Tectal plate glioma, pineal tumour, posterior fossa tumours.
Idiopathic (called late-onset idiopathic aqueductal stenosis).
IMAGING:
- MRI is considered a superior imaging modality as it better delineates the extent of obstructive hydrocephalus with marked enlargement of the lateral and third ventricles. The 4th ventricle is not dilated.
- The aqueduct may show funnelling superiorly.
- In cases of secondary obstruction, the underlying abnormality may also be evident (e.g. web, tumour).
- Sagittal T2: the absence of flow-void signal intensity at the aqueductal level has been suggested as a sign of aqueductal stenosis.
- Sagittal CISS: best demonstrates the obstructing web.
- CSF flow study: decreased aqueductal stroke volume and peak systolic velocity.
Dr. Chanabasappa. V. Chavadi
Senior Consultant
Department of Radiology
Manipal hospital, Sarjapur road, Bengaluru.
Dr. C. Vaishali Raj
Cross Section Fellow
Manipal hospital, Bengaluru.

