
A 20 years old male patient presented with history of trauma to right eye followed by diplopia.
A 20 years old male patient presented with history of trauma to right eye followed by diplopia.
FINDINGS:
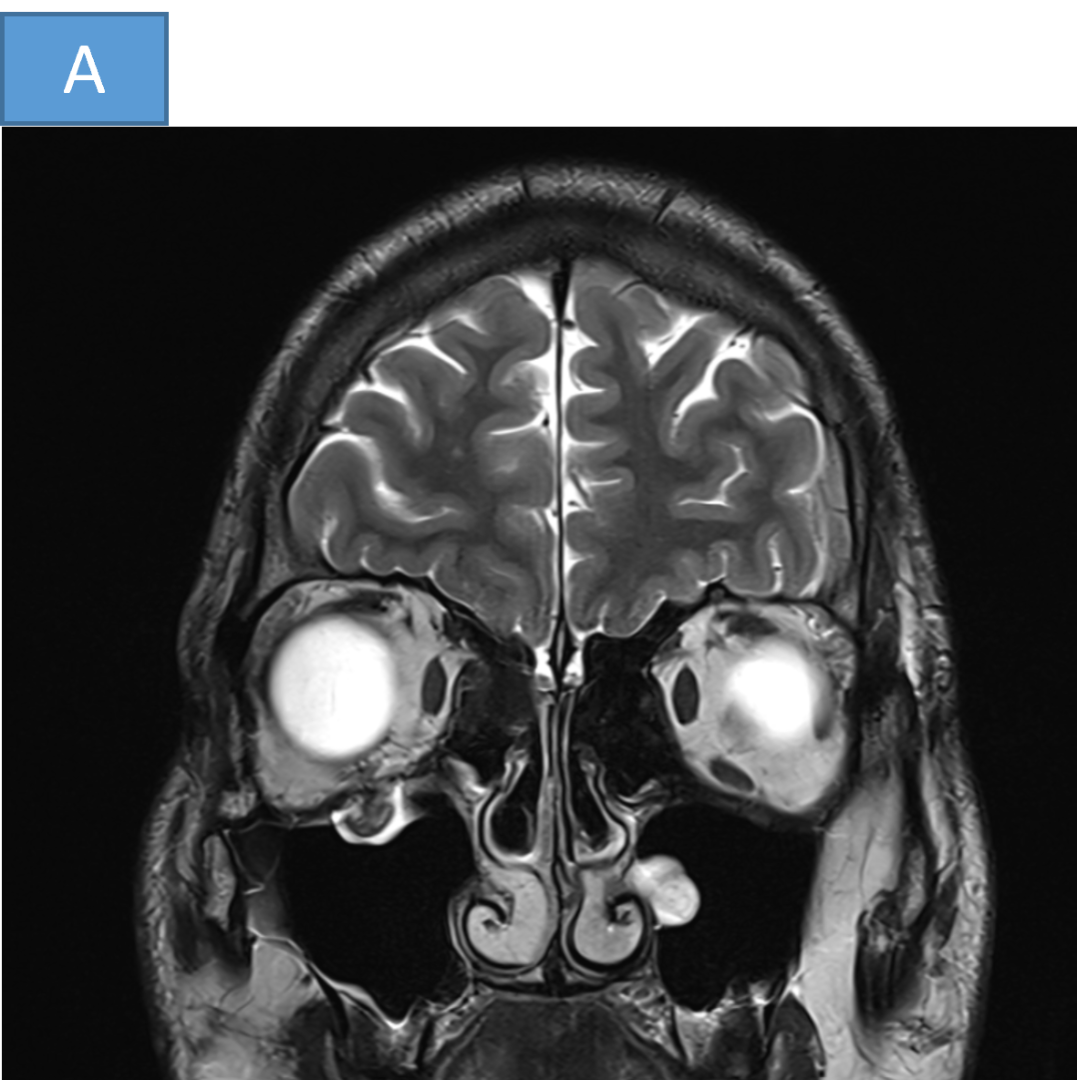
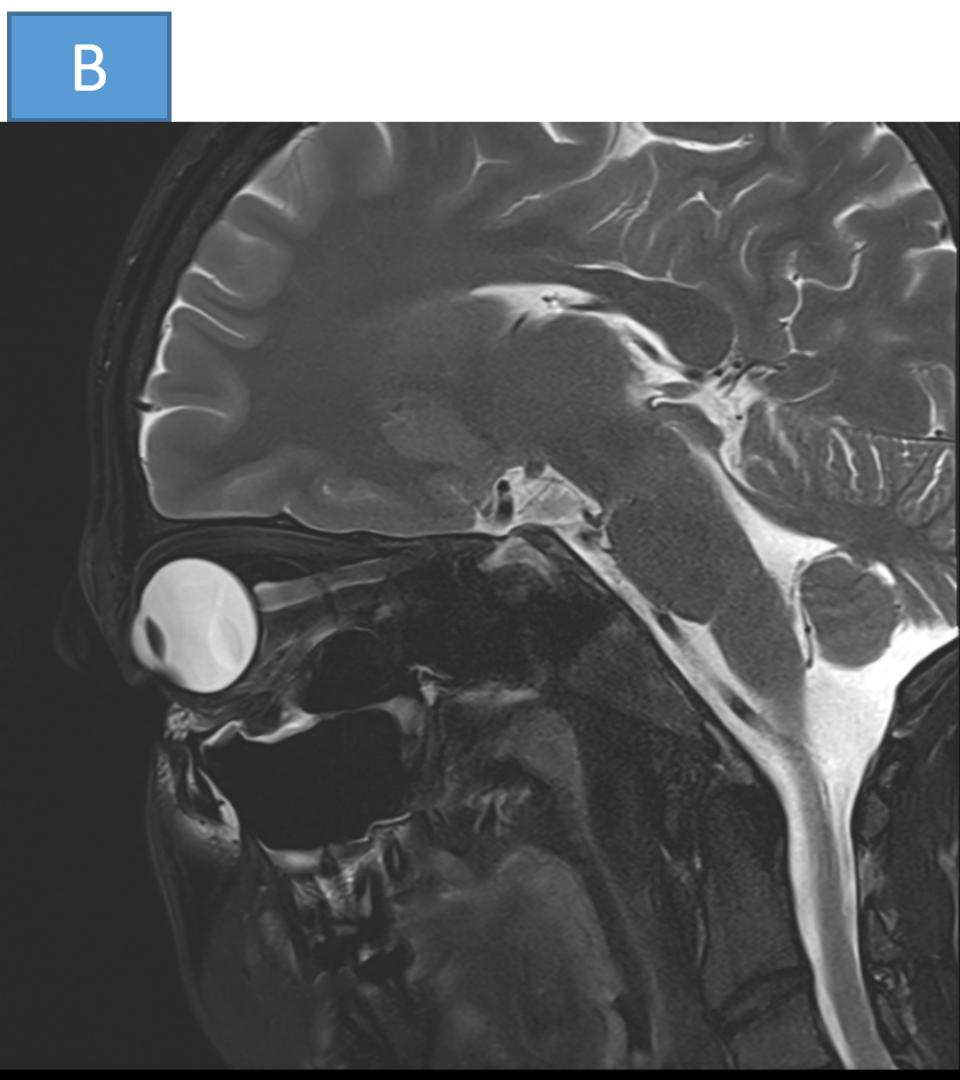
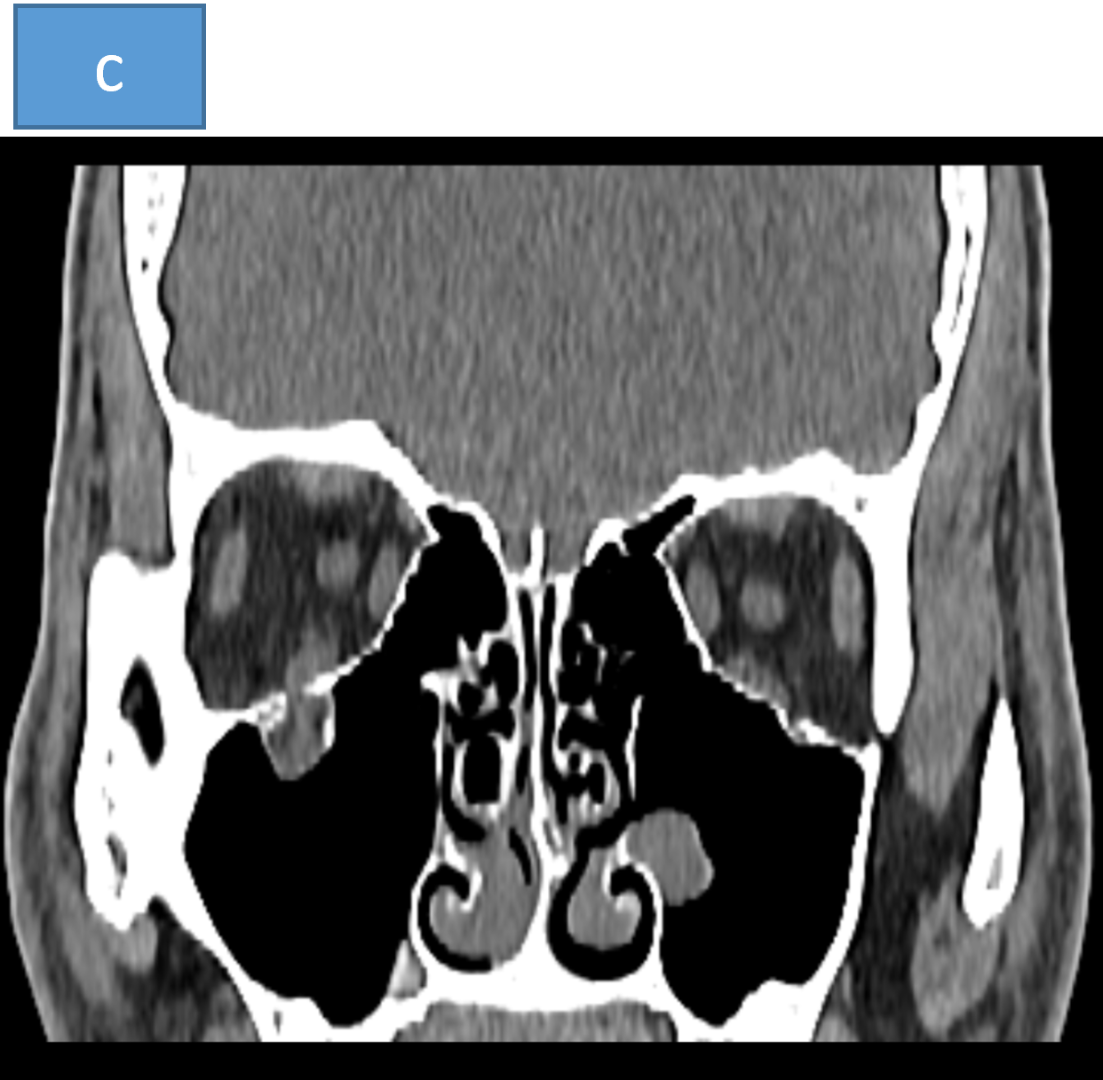
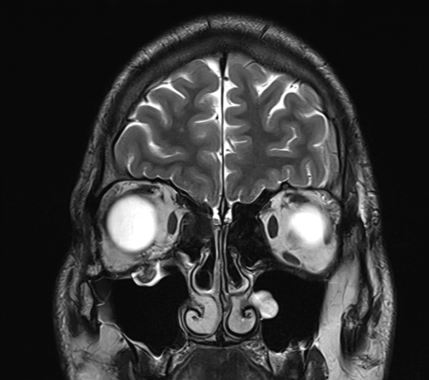
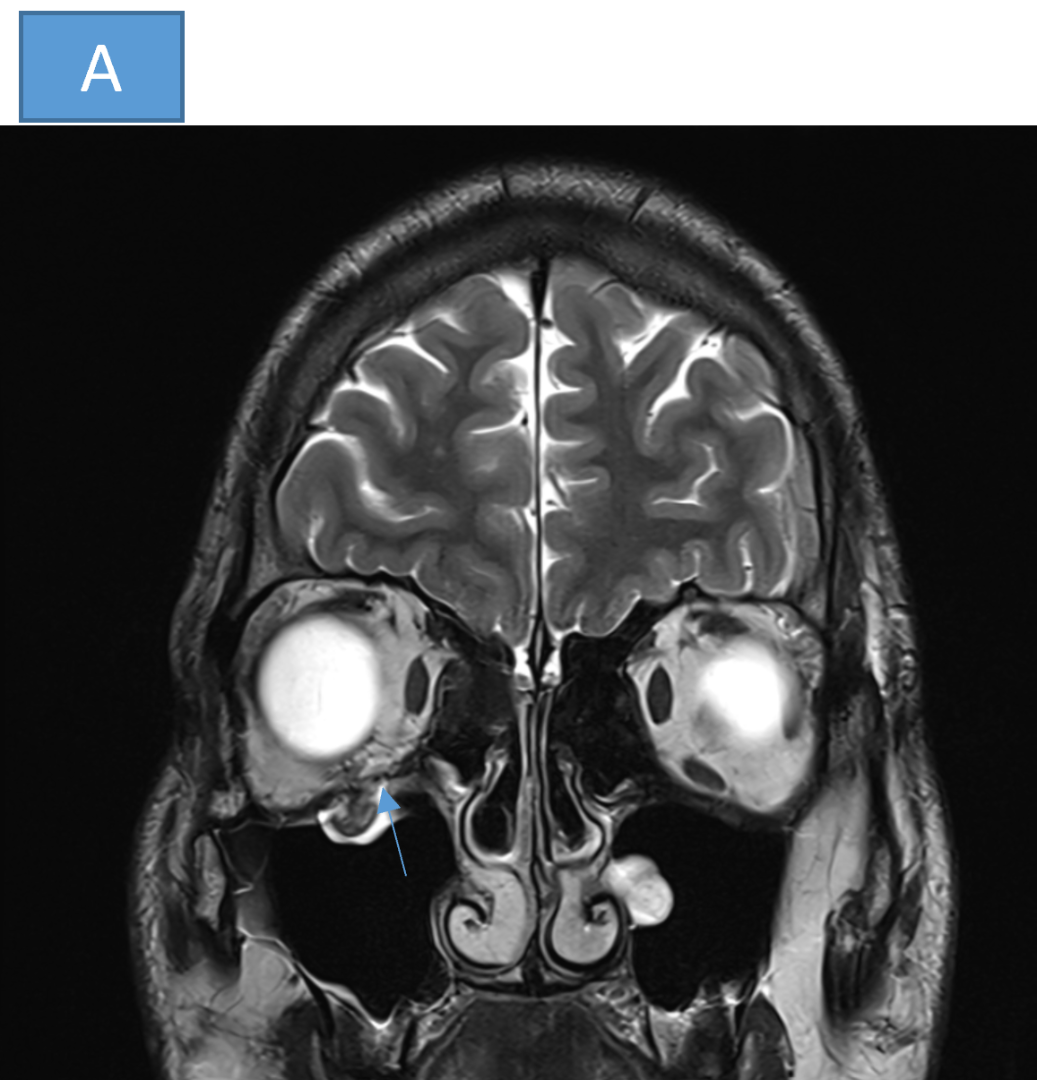
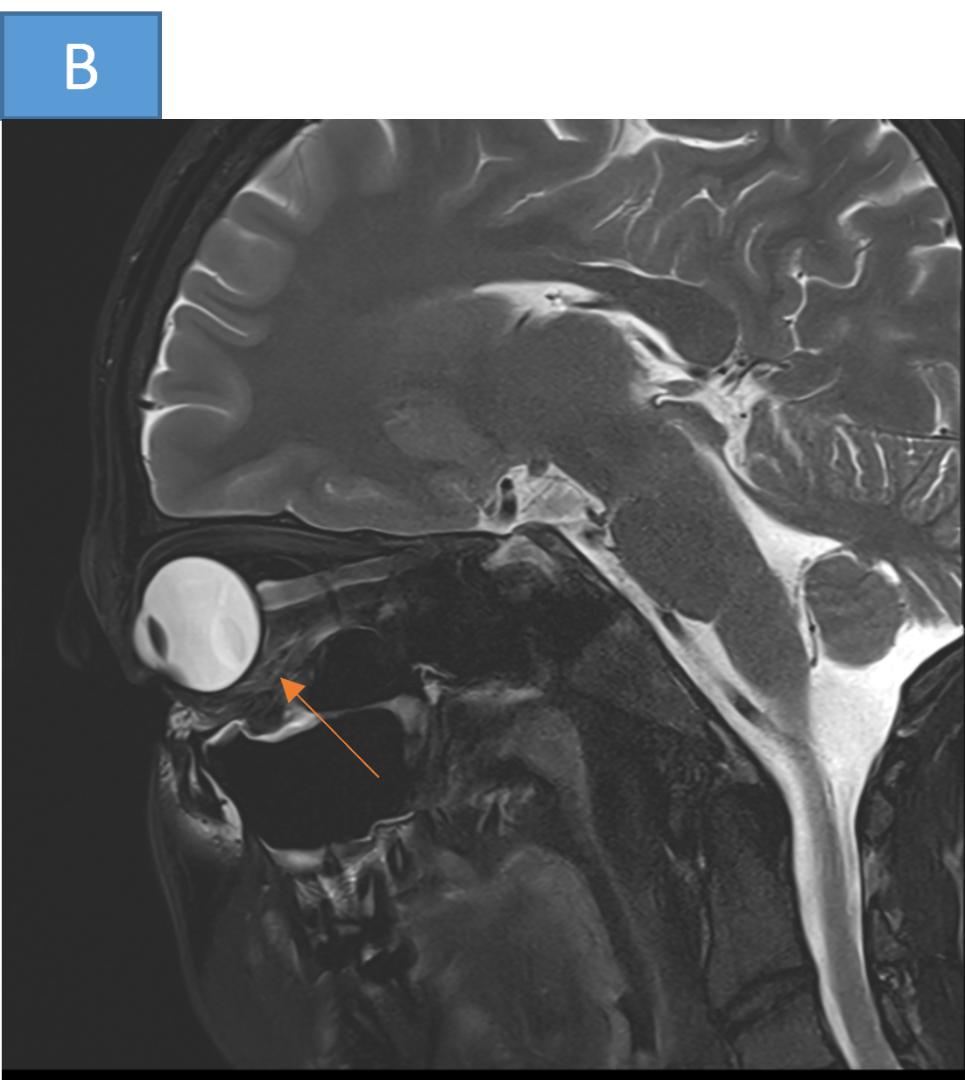
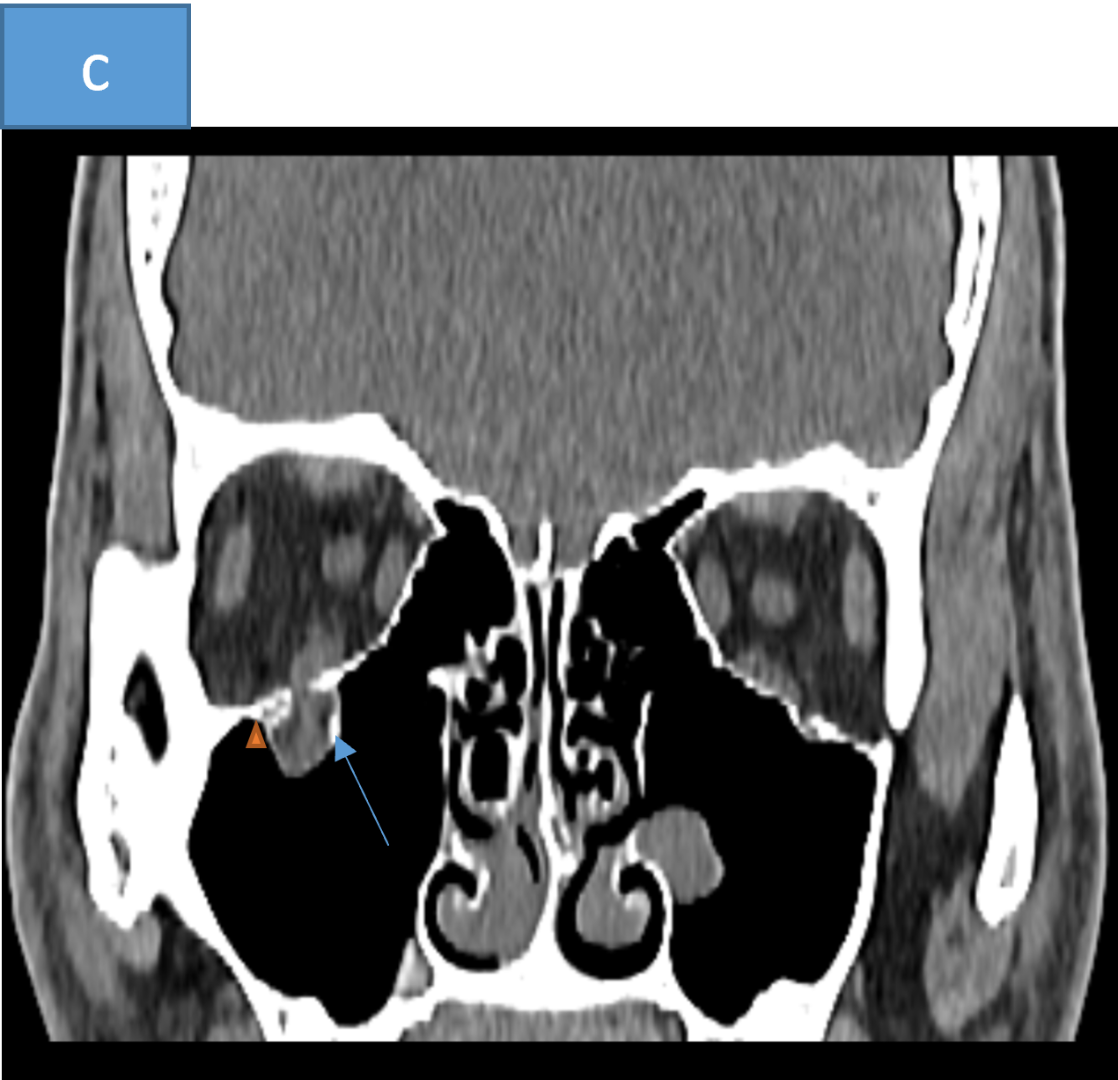
MRI and CT images demonstrate a displaced fracture, running in the sagittal plane, through the floor of the right orbit (blue arrow), just medial to the infra-orbital canal (arrow head). The inferior rectus muscle is entrapped within the defect. There is an associated angulation seen within the inferior rectus on the sagittal images (orange arrow).
DIAGNOSIS:
- Orbital blow-out fracture
DISCUSSION:
Orbital blow-out fracture
- Orbital blow-out fractures occur when there is a fracture of one of the walls of orbit but the orbital rim remains intact. This is typically caused by a direct blow to the central orbit from a fist or ball.
Clinical features:
Orbital blow-out fractures are usually the result of a direct blow to the orbit, which causes a sudden increase in intraorbital pressure. Decompression then occurs by fracture of one or more of the bounding walls of the orbit.
Clinical findings associated with orbital blow-out fracture may include:
- Enopthalmos : due to increased orbital volume.
- Diplopia: due to extraocular muscle entrapment.
- Orbital emphysema : especially when the fracture is into an adjacent paranasal sinus.
- Malar region numbness: due to injury to the infraorbital nerve.
- Hypoglobus.
Blow-out fractures can occur through one or more of the orbital walls:
- Inferior (floor)
- Medial wall (lamina papyracea)
- Superior (roof)
- Lateral wall
Inferior blow-out fracture:
- Orbital fat prolapses into the maxillary sinus and may be joined by prolapse of the inferior rectus muscle. In children, the fracture may spring back into place ( trapdoor fracture). Most fractures occur in the floor posterior and medial to the infraorbital groove.
Medial blow-out fracture:
- Medial blow-out fractures are the second most common type, occurring through the lamina papyracea. Orbital fat and the medial rectus muscle may prolapse into the ethmoid air cells.
Superior blow-out fracture:
- Pure superior blow-out fractures (without associated orbital rim fracture) are uncommon. They are usually seen in patients with pneumatization of the orbital roof.
Lateral blow-out fracture:
- Pure lateral blow-out fractures are rare, as the bone is thick and bounded by muscle. If fractures are present they are usually associated with orbital rim or other significant craniofacial injuries.
Imaging:
Plain radiograph
- Fractures involving the inferior or medial wall may be suspected by visualization of fluid within the maxillary sinus and ethmoidal air cells, respectively.
- Other signs of a blow-out fracture are air within the orbit (which has entered from the maxillary or ethmoid sinuses), an indistinct orbital floor on occipitomental views and opacification of the sinuses due to blood within them. An air-fluid level may be seen in the maxillary sinus.

Air-fluid level in the right maxillary antrum associated with a "tear drop" arising from the orbital floor consistent with prolapsed orbital content
CT:
CT is the modality of choice for the assessment of the facial skeleton. In addition to evaluating the location and extent of fractures, other features requiring assessment and report include:
- Presence of intraorbital (usually extraconal) hemorrhage: may result in stretching or compression of the optic nerve.
- Globe injury/rupture.
- Extraocular muscle entrapment: suspected if there is an acute change in angle of the muscle.
- Prolapse of orbital fat.
Several imaging features are associated with late enophthalmos :
- Surface area of fracture ≥2 cm.
- ≥25-50% involvement of inferior or medial orbital walls.
- Collapse of internal orbital buttress or convex junctional bulge.
- Intraorbital soft tissue herniation volume ≥1.5 mL.
References:
- Orbital blow-out fracture | radiology reference article | radiopaedia.org. Available at: https://radiopaedia.org/articles/orbital-blow-out-fracture-lang=us (Accessed: 05 November 2024).
- Orbital blow-out fracture, eurorad/ DO10.1594/EURORAD/CASE.1547
Dr. HARSHA CHADAGA DMRD,DNB,PDCC,EDiNR
Senior consultant radiologist and HOD of radiology
Manipal Hospital Radiology Group , yeshwanthpur, bengaluru.
Dr. VASANTH KUMR L MDRD
Fellow in cross sectional imaging
Manipal Hospital , yeshwanthpur, bengaluru.
