
A 16 years old male presented with complains of reduced hand grip, reduced sensation over the medial aspect of little and ring fingers bilaterally(right>left) for the past 3 months on left and for the past 6 months on right.
- A 16 years old male presented with complains of reduced hand grip, reduced sensation over the medial aspect of little and ring fingers bilaterally(right>left) for the past 3 months on left and for the past 6 months on right.
- H/o worsening of symptoms during cold exposure.
- O/E
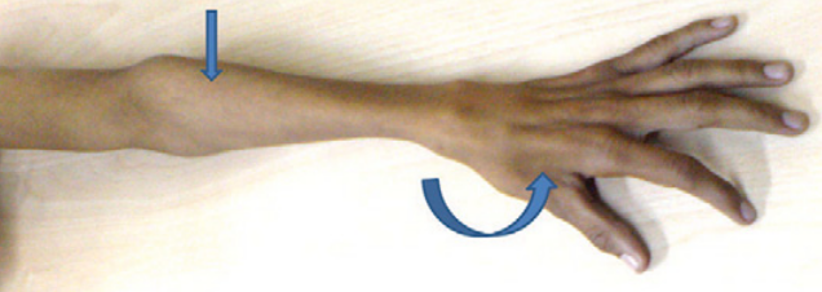
- Wasting of the hypothenar muscles(right > left) and medial forearm muscles of right upper limb.
- Weakness of muscles of hand and forearm (right > left) along the ulnar nerve innervation.
- Polyminimyoclonus present involving the right sided fingers.
- Sensation over right little, ring finger and over hypothenar eminence reduced by 30 percent for touch.
- Reflexes- Biceps 1+, triceps 1+ and supinator not elicitable.
- Lower limbs examination were normal.
- No palpable thickening of nerves of the upper limbs.
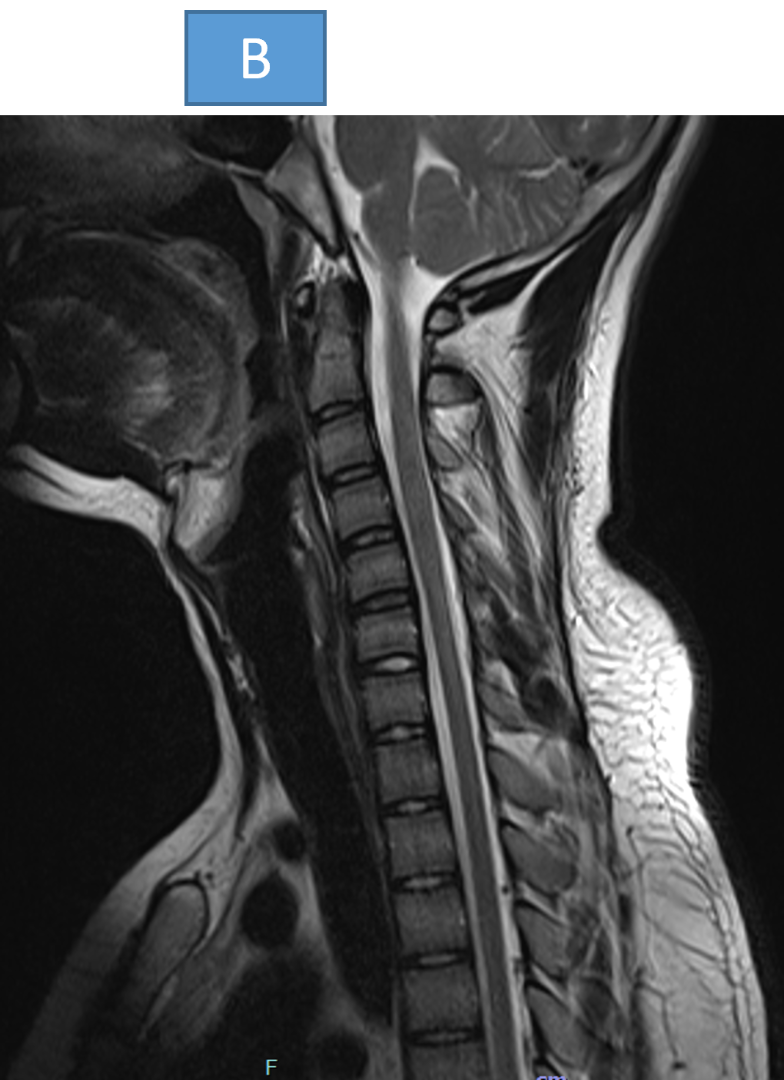
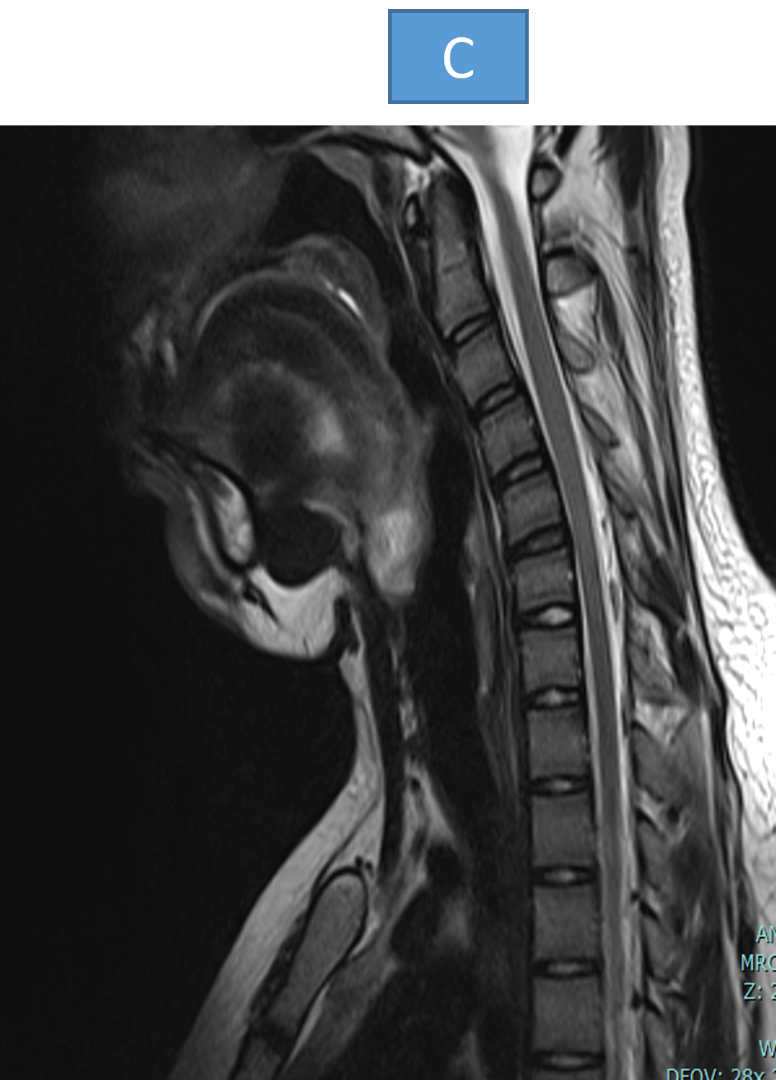
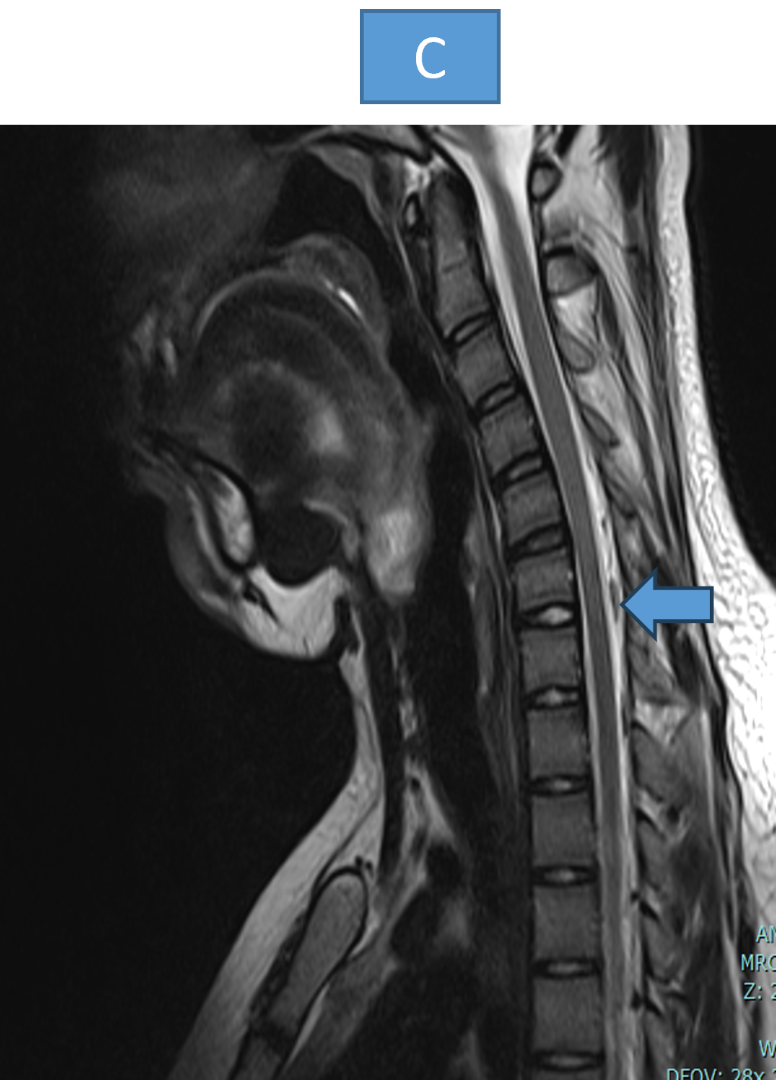
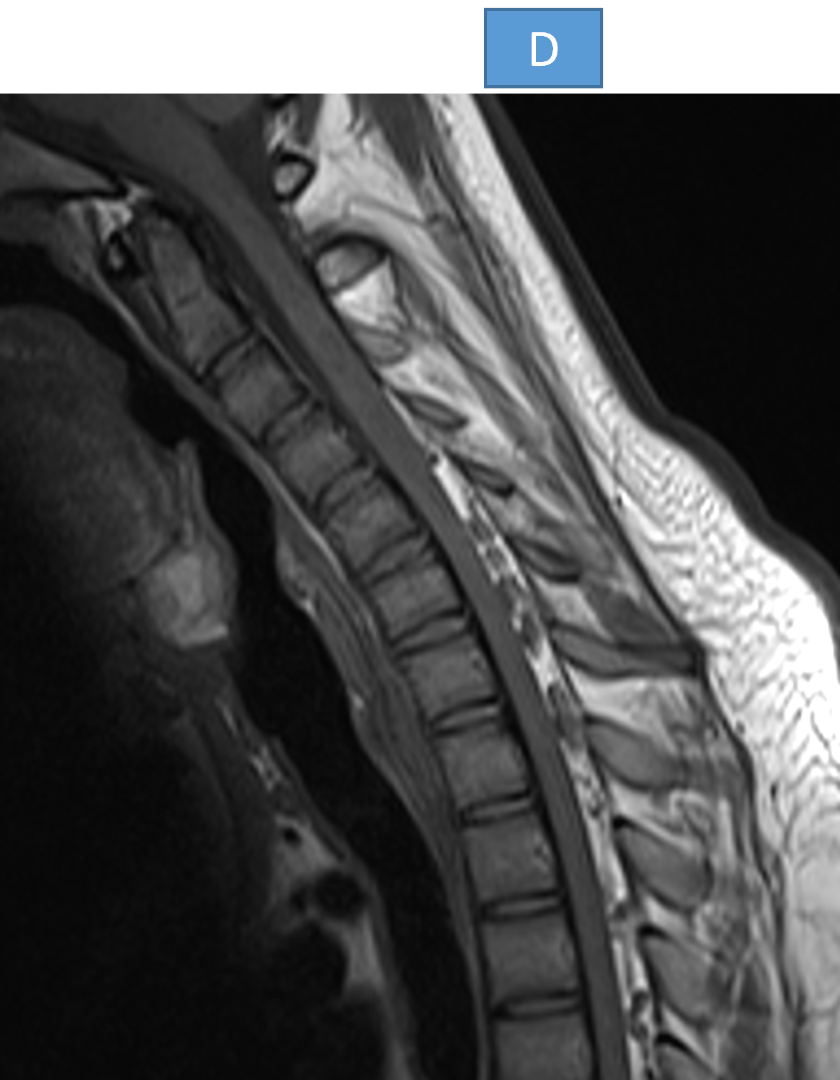
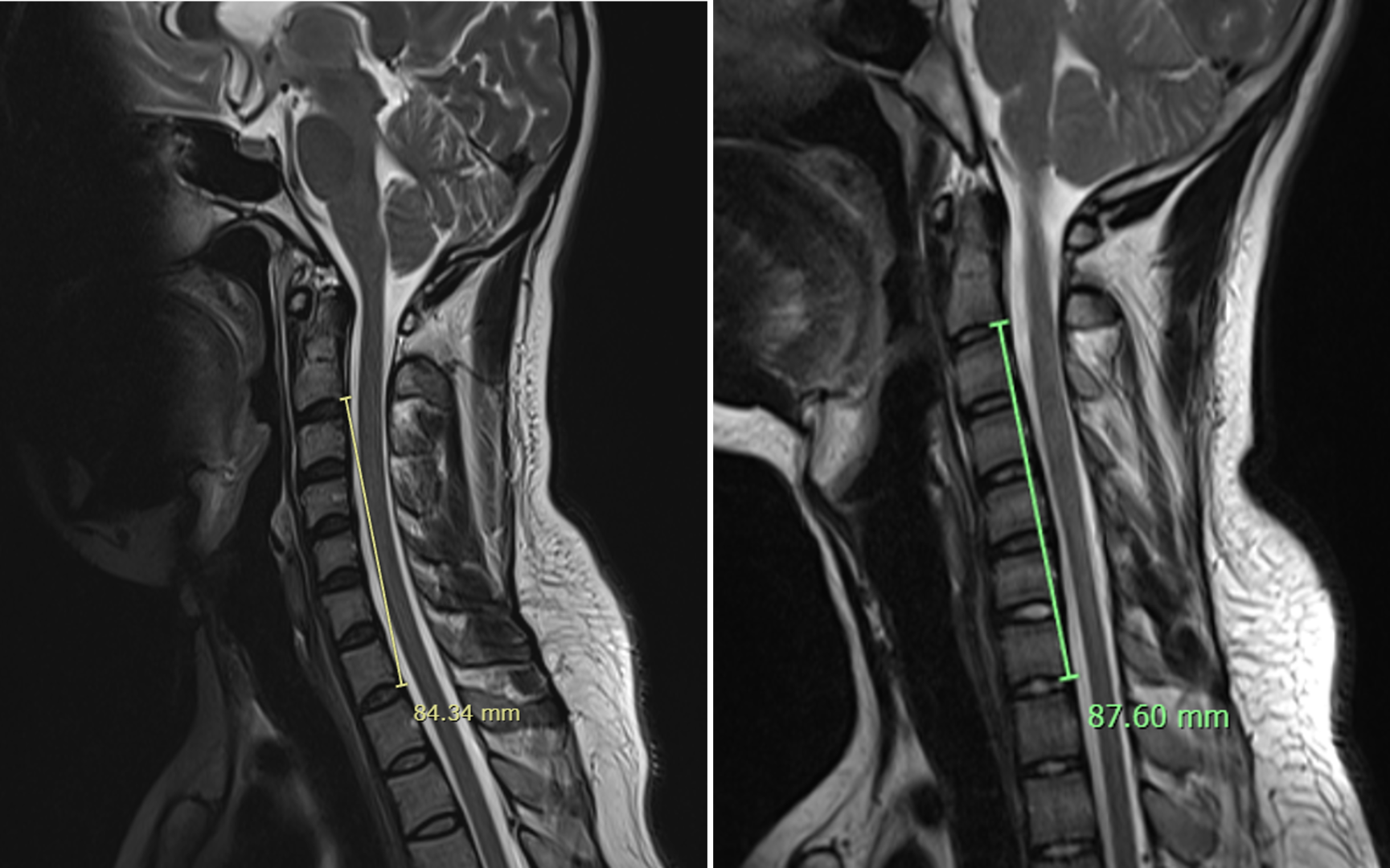
- Patients underwent contrast MRI of cervical spine with flexion and extension dynamic sequences.
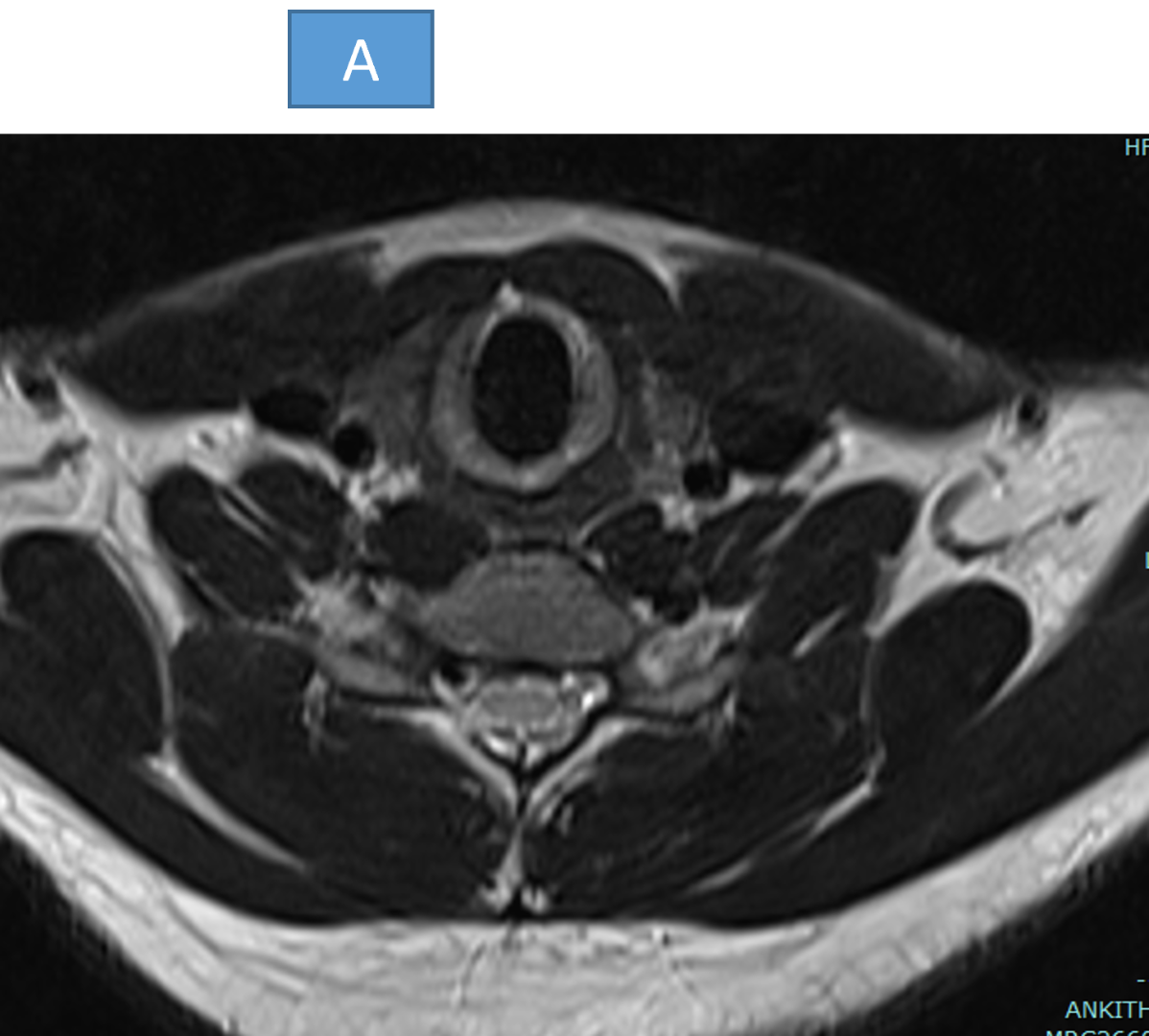
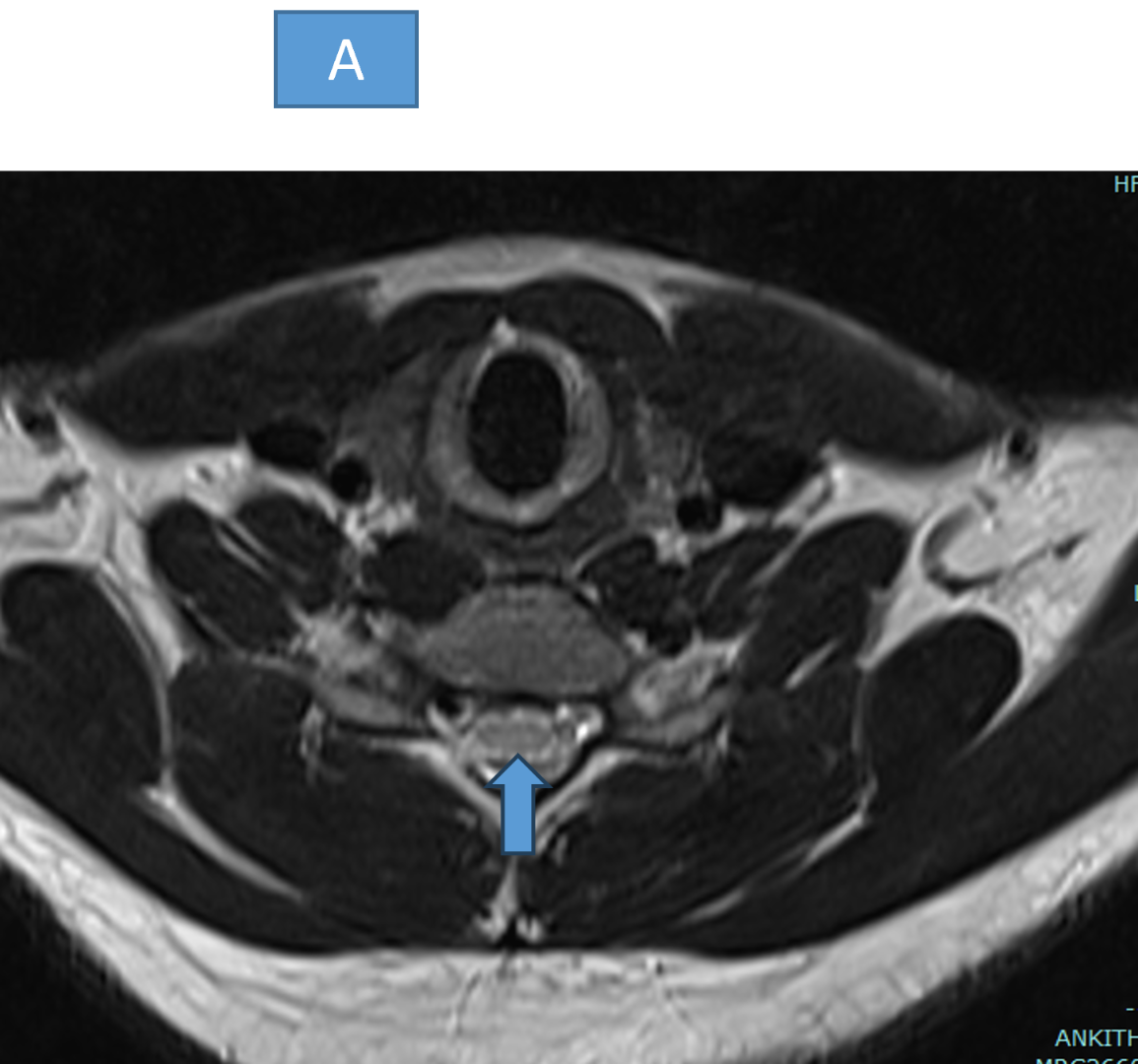
- There is mild intramedullary hyperintensity seen involving central and posterior aspect of cord at C4-C6 level (arrow in A)
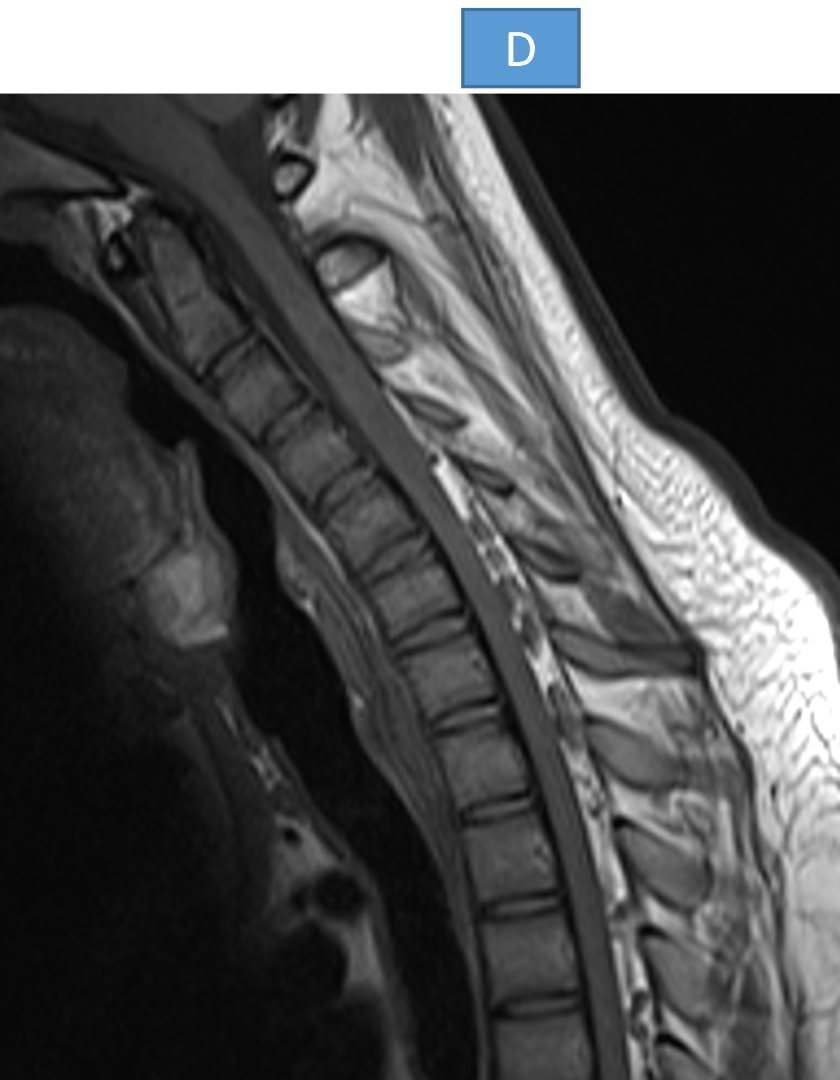
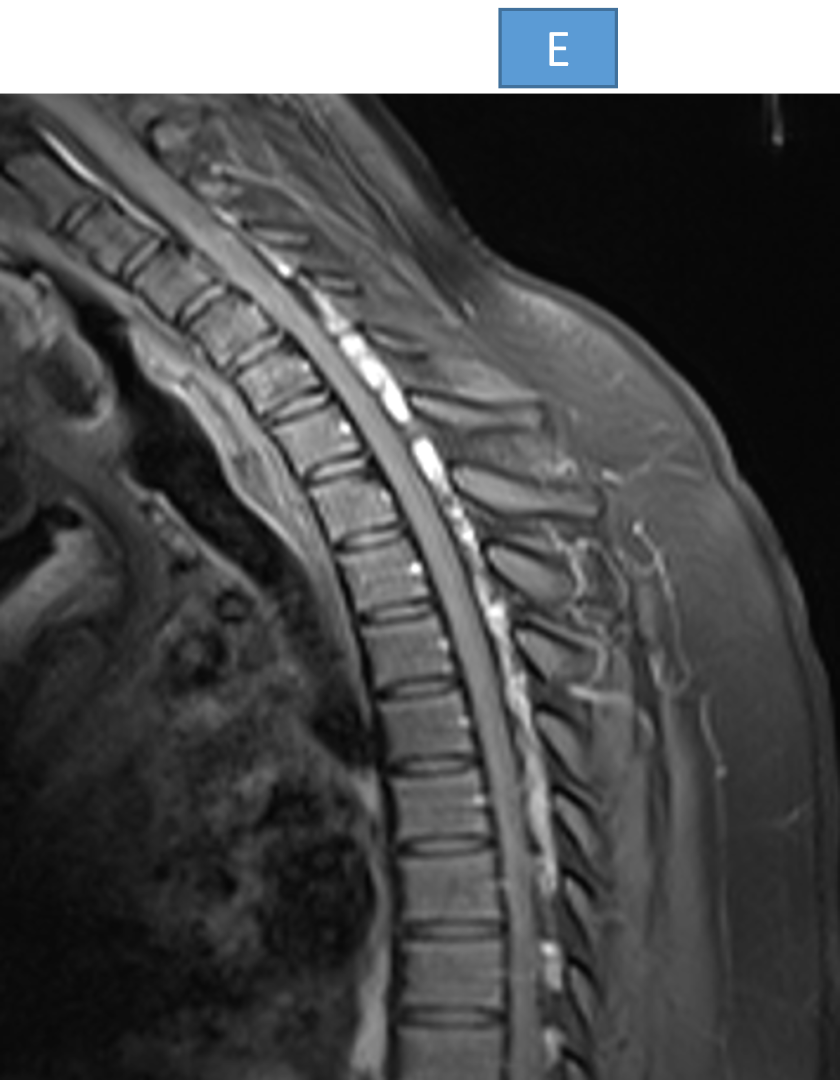
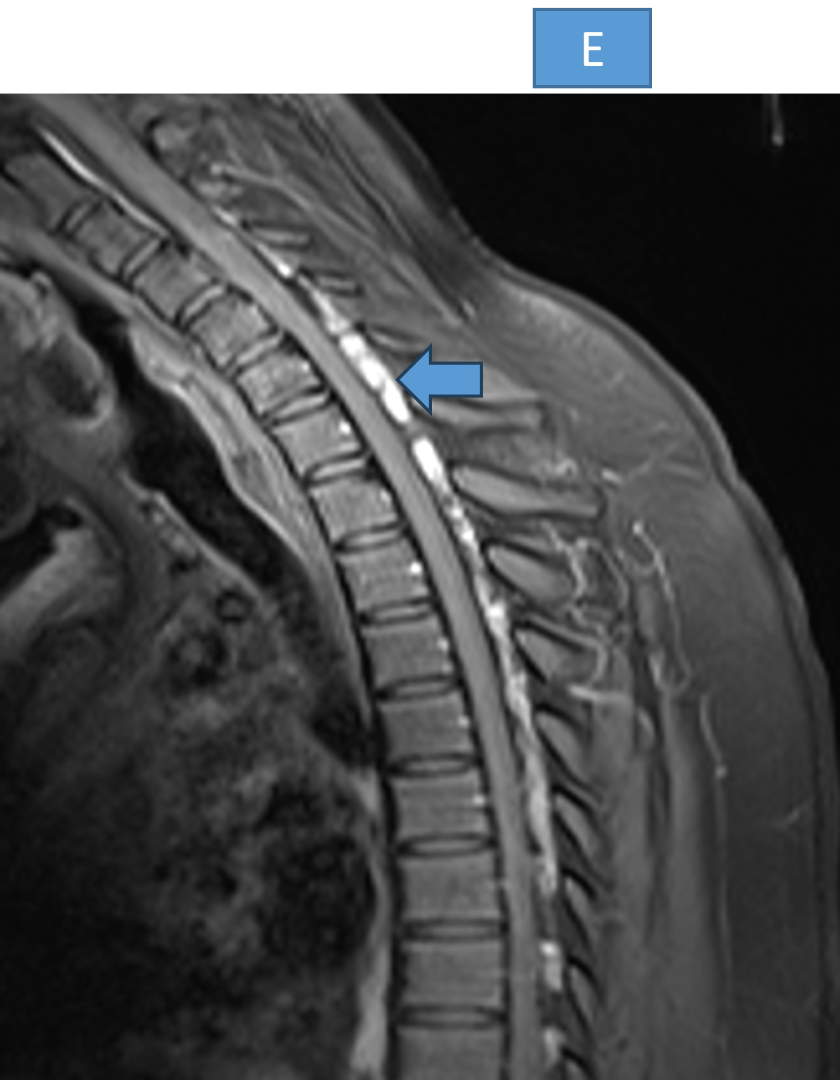
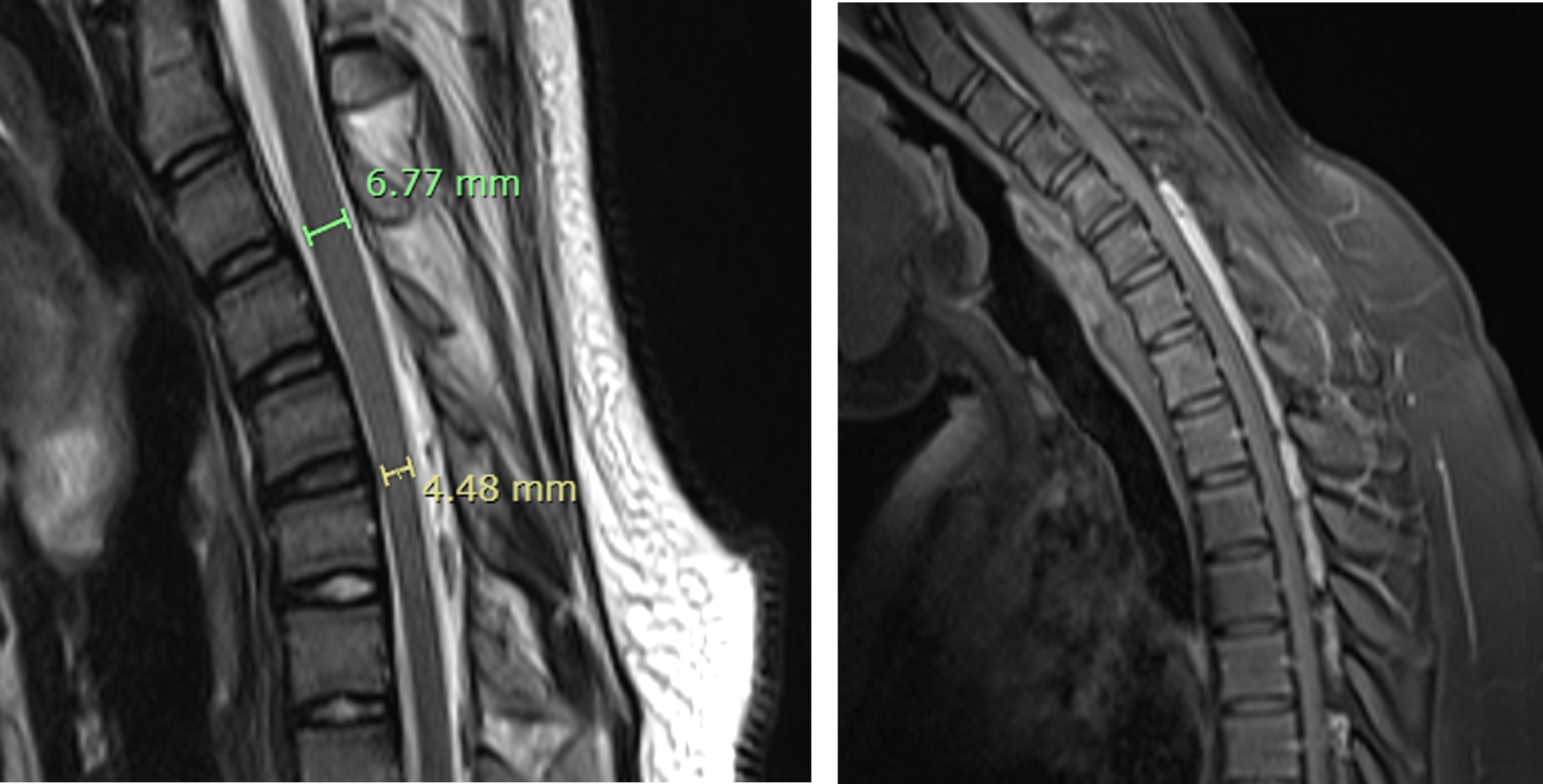
- Mild anterior displacement of the posterior dura seen on flexion sagittal images (arrow in C) with homogenous enhancement and internal flow voids extending from the level of inferior endplate of C4 to inferior endplate of D4.
- Mild anterior displacement of the posterior dura seen on flexion sagittal images with homogenous enhancement and internal flow voids extending from the level of inferior endplate of C4 to inferior endplate of D4 ( arrow in E)
Hirayama disease
- Benign self limiting cervical myelopathy/upper motor neuron disease affecting young adults in the age group of 20–30 years.
- Results from “Tight dural canal”.
Terminologies:
- Monomelic amyotrophy or
- Non-progressive juvenile spinal muscular atrophy of the distal upper limbs.
Clinical presentation
- Patients present with progressive unilateral, upper limb myopathy in the form of weakness and tremors.
- Muscles of the forearm and hand are affected, sparing brachioradialis, giving the characteristic appearance of oblique amyotrophy that affects the C7, C8 and T1 myotomes.
- Cold paresis : Exacerbating of finger weakness on exposure to cold environment
- No sensory or pyramidal tract involvement. The amyotrophy is unilateral in most patients, asymmetrically bilateral in some and rarely symmetric.
Pathology
- Chronic microcirculatory changes in the territory of the anterior spinal artery induced by repeated or sustained flexion account for the necrosis of the anterior horns of the lower cervical cord.
- The disease usually arrests after 3-5 years
Radiographic features
Neutral MRI
- Loss of normal cervical lordosis with straight or kyphotic cervical spine
- Loss of attachment between the posterior dural sac and subjacent lamina,
- Localized lower cervical cord atrophy/Cord flattening,
- Non-compressed short segment intramedullary high signal intensity on T2-weighted MR images
Flexion position
- Forward migration of the posterior wall of the lower dura.
- Enlarged posterior epidural space which appears crescentric appears as high signal intensity on T1- and with or without epidural flow voids.
- At the site of maximal forward shift of the posterior dural sac, the spinal cord is dynamically compressed with reduced AP diameter.
- enhances uniformly on T1 C+ (Gd).
Reference
- Hirayama Flexion Myelopathy: Neutral-Position MR Imaging Findings—Importance of Loss of Attachment. Chi-Jen Chen Endometrial thickness at al. 10.1148/radiol.2311030004 Radiology 2004; 231:39–44.
Dr Pravin Kumar M
MBBS, DMRD, DNB
Senior Consultant Manipal Hospitals Radiology Group Hebbal.
Dr Vasanth kumar L
MBBS, M.D.
Cross section imaging fellow - MHRG

