
A 16 month old baby with bilateral sensorineural hearing loss
A 16-month-old baby with bilateral sensorineural hearing loss
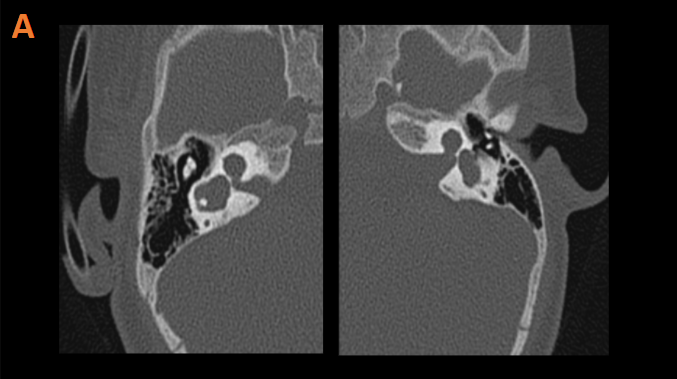
A. Dysplastic cochlea bilaterally (Blue solid arrow).
Dilated and dysplastic vestibule bilaterally (Orange solid arrow).
Absent modiolus bilaterally (Green arrow).
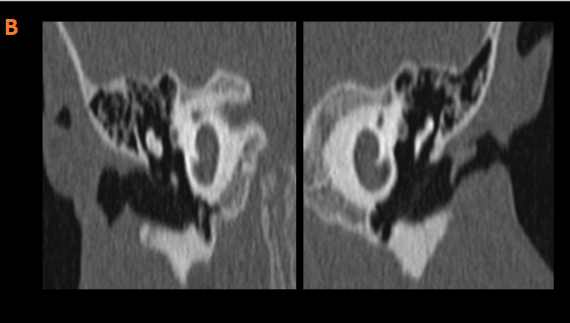
B. Fused apical and middle turns of cochlea bilaterally with dilated basal turn.
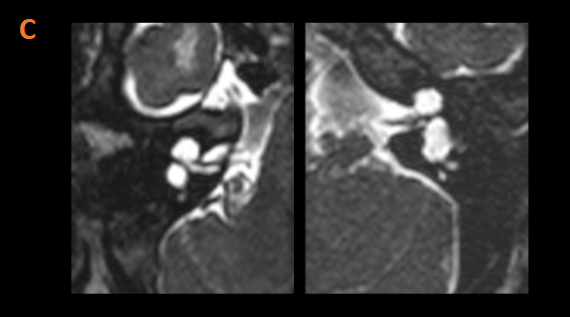
C. Patent and dilated cochlear aperture bilaterally.
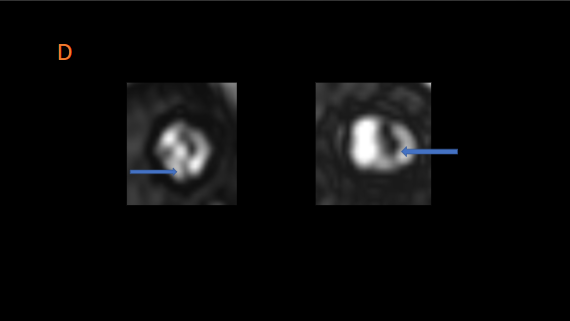
D. RIGHT – The cochlear nerve is present but appears hypoplastic.
LEFT – The cochlear nerve is not separately visualized.
The vestibulocochlear nerve is seen as a single complex.
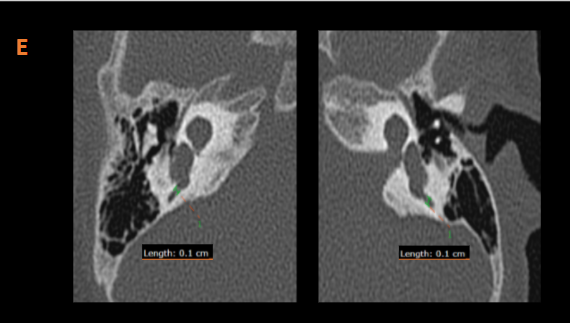
E. Vestibular aqueduct is not dilated.
DIAGNOSIS:
Bilateral vestibulocochlear malformation, most likely representing bilateral type I incomplete partition.
DISCUSSION:
- Incomplete partition anomalies are the most common group constituting more than 40%.
- These anomalies are characterized by incomplete partition of cochlea, deficiencies in the interscalar septum and/or modiolus in varying degree of severity.
- However there is clear differentiation between cochlea and vestibule; and the size of cochlea is normal.
- There are 3 subtypes
- Incomplete partition Type I also known as cystic cochleovestibular malformation,
- Incomplete partition Type II associated with enlarged vestibule aqueduct and mildly dilated vestibule, the triad is known as Mondini malformation.
- Incomplete partition Type III observed in X-linked deafness.
- Type I incomplete partition is also known as cystic cochleovestibular malformation. It most likely results from a developmental arrest in the 5th week of gestation. The modiolus is entirely absent; the cochlea has a cystic appearance; and the vestibule is often dilated, forming a figure eight. The fact that the vestibule is distinguishable from the cochlea makes it possible to differentiate a type I incomplete partition from a common cavity. The vestibular aqueduct is normal. The cribriform area between the cochlea and IAC is often defective, and all patients have a large IAC, predisposing them to increased risks for meningitis and for a perilymphatic gusher in the event of surgery. Type I incomplete partition is less well differentiated than type II incomplete partition.
DIFFERENTIALS:
- Common cavity: the cochlea and vestibule are also cystic but they are not separated.
- Incomplete partition Type II: Cochlea with normal basal turn and cystic apex; strong association with enlarged vestibular aqueduct.
References:
1. CT and MR Imaging of the Inner Ear and Brain in Children with Congenital Sensorineural Hearing Loss- Varsha M. Joshi et al.
2. Classification and Current Management of Inner Ear Malformations- Levent Sennaro?lu, and Münir Demir Bajin
3. The link between inner ear malformations and the rest of the body: what we know so far about genetic, imaging and histology- Felice D’Arco et al.
Dr Anita Nagadi
MD, MRCPCH, FRCR
Senior Consultant Radiologist
Manipal Hospital, Yeshwanthpur
Dr Soham Naik
MDNB resident
Manipal Hospital, Yeshwanthpur
