
A 13-year old pre-menarchal girl, with features of excess acne and hirsuitism
A 13-year old pre-menarchal girl, with features of excess acne and hirsuitism
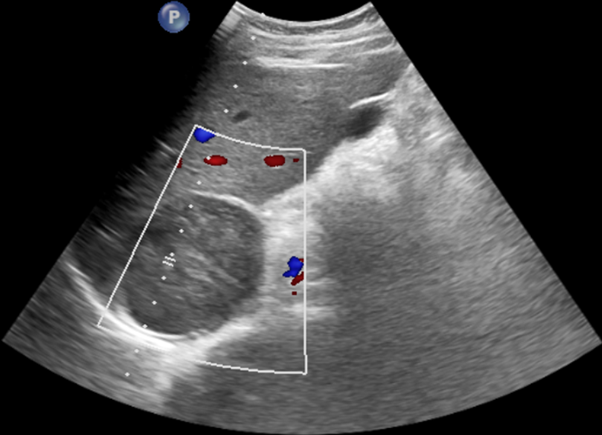
- Ultrasound demonstrates a uniformly hypoechoic right suprarenal mass.
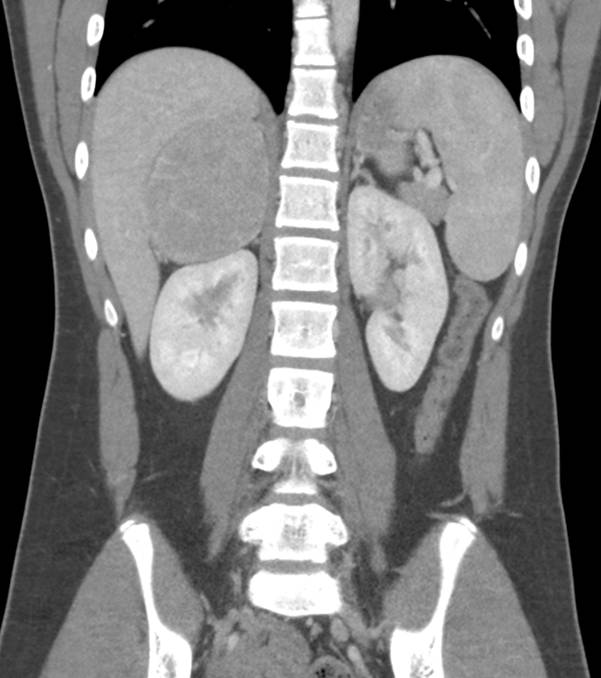
- CECT Abdomen and Pelvis coronal image demonstrates a well-defined homogeneously enhancing mass lesion (~7 cm in size) arising from the right adrenal gland and indenting the right kidney and liver with no infiltration into adjacent structures.
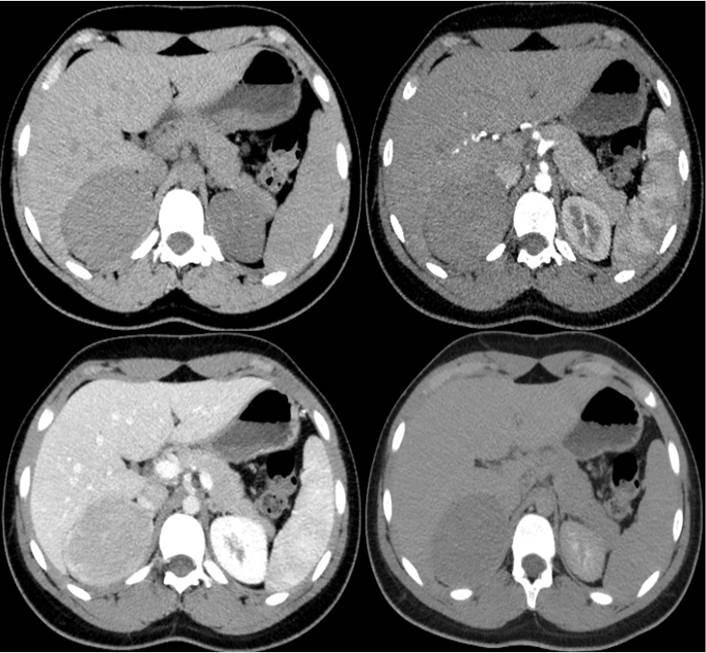
- Non-contrast axial images demonstrate increased attenuation of adrenal lesion measuring 45 HU with further axial arterial, venous, and 15-minute delayed images demonstrating Absolute Percentage Washout (APW) of 75 % and Relative Percentage Washout (RPW) of 43 %.
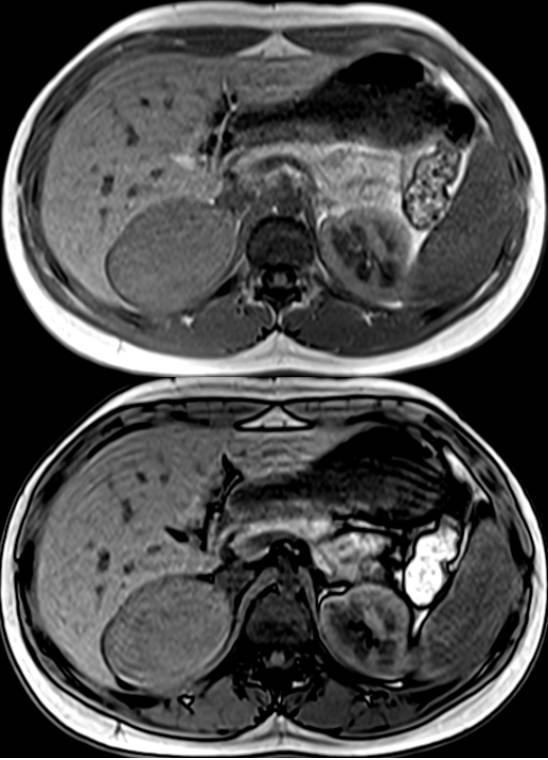
- On MRI, In and Out of phase images, no significant chemical shift artifact was observed.
- Gross pathology post-operative specimen shows a smooth encapsulated mass.
- HPE – The tumor is composed of cells with pink cytoplasm and focal cells with clear cytoplasm. The cells are arranged in nests and show significant nuclear pleomorphism with a few cells showing large bizarre nuclei and prominent nucleoli. Apoptosis and occasional mitoses were seen. There is no capsular/ vascular invasion. No necrosis was seen.

Diagnosis:
Lipid poor functioning right adrenal cortical adenoma.
Discussion:
- Most adrenal lesions are non-functional and benign, and are usually incidentally diagnosed. Only a small number of adrenal tumors are functional and even smaller number are malignant lesions.
- Functioning adrenal lesions can be:
- Adrenal cortex – Adrenal cortical hyperplasia, Adrenal adenoma, Aldosteronoma or Adrenal cortical carcinoma.
- Adrenal medulla – Phaeochromocytoma.
- In this case, blood parameters demonstrated increased cortisol levels and increased male hormonal levels (androgen) suggesting a dual hormone secreting adrenal lesion.
- No cushingoid features or abnormal blood pressure.
Lipid Poor Functioning Adrenal Adenoma:
- Characterisation of adrenal adenomas can be based on anatomical features i.e, increased intracellular lipid content (Average < 10 HU) and physiologic vascular enhancement pattern using dynamic contrast protocol demonstrating an APW > 60%, which has a sensitivity of 88 % and specificity of 96 %, and RPW > 40 %, which has a sensitivity of 83 % and specificity of 93 %.
- Nearly 30 % of adenomas lack sufficient intracellular lipid content and if non contrast CT demonstrates a HU value of > 20 -30 HU, chemical shift MR imaging may be less useful in arriving to a diagnosis of an adenoma.
- Delayed (15 min) enhanced CT can help characterize hyperattenuating adrenal masses that cannot be characterized with chemical shift MR imaging.
Differential diagnosis:
- Adrenal cortical carcinoma: Large irregular heterogenous mass with necrosis and infiltration adjacent structures.
- Phaeochromocytoma: Intense enhancement in arterial phase, demonstrates washout pattern similar to adenoma and appears as T2 hyperintense lesion (lightbulb sign) on MRI.
- Adrenal metastases.
References:
- Albano D, Agnello F, Midiri F, et al. Imaging features of adrenal masses. Insights Imaging. 2019;10(1):1. Published 2019 Jan 25. doi:10.1186/s13244-019-0688-8
- Caoili EM, Korobkin M, Francis IR, Cohan RH, Dunnick NR. Delayed enhanced CT of lipid-poor adrenal adenomas. AJR Am J Roentgenol 2000;175:1411–1415.
- Park, B. K., Kim, C. K., Kim, B., & Lee, J. H. (2007). Comparison of Delayed Enhanced CT and Chemical Shift MR for Evaluating Hyperattenuating Incidental Adrenal Masses1. Radiology, 243(3), 760–765. doi:10.1148/radiol.2433051978
Dr. Diwakar C
Radiology Resident,
Manipal Hospitals Radiology Group.
Dr. Vivek Jirankali MD,
Senior Resident and Cross-Sectional Fellow,
Manipal Hospitals Radiology Group.
